DEFINITIONS
DEFINITIONS
Action
potential
http://en.wikipedia.org/wiki/Action_potential
An action potential is a "spike" of electrical
discharge that travels along the membrane of a cell.
Action potentials are an essential feature of animal
life, rapidly carrying information within and between tissues.
They also occur in some plants. Action potentials can be created by many types
of cells, but are used most extensively by the nervous
system for communication between neurons
and for transmitting information from neurons to other body tissues such as muscles
and glands.
Action potentials are not the same in all cell types and can even vary in their
properties at different locations in the same cell. For example, cardiac action potentials
are significantly different from the action potentials in most neurons. This
article is primarily concerned with the "typical" action potential of
axons.
http://en.wikipedia.org/wiki/Active_listening
When interacting,
people often are not listening attentively to one another. They may be
distracted, thinking about other things, or thinking about what they are going
to say next, (the latter case is particularly true in conflict situations or
disagreements). Active listening is a structured way of listening and
responding to others. It focuses attention on the speaker. Suspending one’s own
frame of reference and suspending judgment, are important in order to fully
attend to the speaker.
Adaptation
(Neural adaptation)
http://en.wikipedia.org/wiki/Neural_adaptation
Neural adaptation or sensory adaptation is a change over time in the responsiveness of the sensory system to a constant stimulus. It is usually experienced as a change in the stimulus. For example, if one rests one's hand on a table, one immediately feels the table's surface on one's skin. Within a few seconds, however, one ceases to feel the table's surface. The sensory neurons stimulated by the table's surface respond immediately, but then respond less and less until they may not respond at all; this is neural adaptation. More generally, neural adaptation refers to a temporary change of the neural response to a stimulus as the result of preceding stimulation. It is usually distinguished from memory, which is thought to involve a more permanent change in neural responsiveness. Some people use adaptation as an umbrella term that encompasses the neural correlates of priming and habituation. In most cases, adaptation results in a response decrease, but response facilitation does also occur. Adaptation is considered to be the cause of perceptual phenomena like afterimages and the motion aftereffect. In the absence of fixational eye movements, visual perception may fade out or disappear due to neural adaptation [1]. (See Adaptation (eye).) While large mechanosensory neurons such as type I/group Aβ will display adaptation, smaller type IV/group C nociceptive neurons do not. As a result, pain does not usually subside rapidly but persists for long periods of time, but one quickly stops receiving touch or other sensory information if surroundings remain constant.
Adaptation is a decrease in sensitivity to
continued stimuli. In fact, the perception of a sensation may actually
disappear even though the stimulus is still being applied. For example, when
you first get into a tub of hot water, you probably feel a burring sensation,
but soon the sensation decreases to one of comfortable warmth even though the
stimulus(hot water) is still present. In time, the sensation of warmth
disappears completely. Other examples of adaptation include placing a ring on
your finger, putting on your shoes or hat, sitting on a chair, and pushing your
glasses up on the top of your head. Adaptation results from a change in a
receptor, a change in a structure associated with a receptor, or inhibitory feedback
from the brain. Receptors vary in their ability to adapt. Rapidly Adapting
(Phasic) receptors such as those associated with pressure, touch, and smell,
adapt very quickly. Such receptors play a major role in signaling changes in a
particular sensation. Slowly adapting (tonic) receptors, such as those
associated with pain, body position, and detecting chemicals in blood, adapt
slowly. These receptors are important in signaling information regarding steady
states of the body.
http://en.wikipedia.org/wiki/Adrenal_gland
http://www.bartleby.com/107/277.html
In mammals, the adrenal
glands (also known as suprarenal glands) are the triangle-shaped endocrine glands that sit on top of the kidneys; their name indicates
that position (ad-, "near" or "at" + -renes,
"kidneys"). They are chiefly responsible for regulating the stress response through the synthesis of
corticosteroids and catecholamines,
including cortisol and adrenaline.
Anatomically, the adrenal glands are located in the thoracic abdomen situated
atop the kidneys,
specifically on their anterosuperior aspect. In humans, the adrenal glands are
found at the level of the 12th thoracic vertebra and receive their blood supply from the adrenal arteries.
Areolar connective tissue
http://en.wikipedia.org/wiki/Areolar_connective_tissue
It can be found in the skin as well as in places that connect epithelium to other tissues. The areolar tissue is found beneath the dermis layer and is also underneath the epithelial tissue of all the body systems that have external openings. It is also a component of mucus membranes found in the digestive, respiratory, reproductive, and urinary systems. It also surrounds the blood vessels and nerves. [edit] Composition It is a pliable, mesh-like tissue with a fluid matrix and functions to cushion and protect body organs. Cells called fibroblasts are widely dispersed in this tissue; they are irregular branching cells that secrete strong fibrous proteins and proteoglycans as an extracellular matrix. The cells of this type of tissue are generally separated by quite some distance by a gel-like gelatinous substance primarily made up of collagenous and elastic fibers [edit] Function It acts as a packaging tissue holding the internal organs together and in correct placement.
It holds organs in
place and attaches epithelial tissue to other underlying tissues. [edit] Classification Loose connective tissue is named
based on the "weave" and type of its constituent fibers. There are
three main types: Collagenous fibers: collagenous fibers are made of collagen and consist
of bundles of fibrils that are coils of collagen molecules. Elastic fibers:
elastic fibers are made of elastin and are "stretchable." Reticular fibers: reticular fibers consist of one or more types of very thin collagen
fibers. They join connective tissues to other tissues.
Afferent
Conveying
impulses toward the central nervous system
Albert
Ellis (1913-2007) (Rational-Emotive Therapy)
http://en.wikipedia.org/wiki/Albert_Ellis
http://changingminds.org/explanations/belief/irrational_beliefs.htm
Albert Ellis (September 27, 1913 – July 24, 2007) was an
American psychologist who in 1955 developed Rational Emotive Behavior Therapy.
He was considered by many to be the grandfather of cognitive-behavioral
therapies and, based on a 1982 professional survey of U.S. and Canadian
psychologists, one of the most influential psychotherapists in history (Carl Rogers
placed first in the survey; Sigmund Freud placed third).[1] Ellis founded and
was the president and president emeritus of the New York City-based Albert
Ellis Institute.[2]
Andrew
Taylor Still (1828-1917)
http://www.meridianinstitute.com/eamt/files/contents.htm
http://www.meridianinstitute.com/eamt/files/still2/st2cont.html
http://en.wikipedia.org/wiki/Andrew_Taylor_Still
Andrew Taylor Still (1828-1917), D.O. wrote in 1899 the
“Philosophy of Osteopathy” [1]
[2] [3]
Andrew Taylor Still (August 6, 1828-December 12, 1917) is
considered the father of osteopathic medicine.[citation needed] Still was born
in Lee County, Virginia in 1828, the son of a Methodist minister and physician.
At an early age, Still decided to follow in his father's footsteps as a
physician. After studying medicine and serving an apprenticeship under his
father, Still became a licensed M.D. in the state of Missouri. Later, in the
early 1860's, he completed additional coursework at the College of Physicians
and Surgeons in Kansas City, Missouri. He went on to serve as a surgeon in the
Union Army during the American Civil War. After the Civil War and following the
death of three of his children from spinal meningitis in 1864, Still concluded
that the orthodox medical practices of his day were frequently ineffective and
sometimes harmful. He devoted the next ten years of his life to studying the
human body and finding better ways to treat disease. His research and clinical
observations led him to believe that the musculoskeletal system played a vital
role in health and disease and that the body contained all of the elements
needed to maintain health if properly stimulated. Still believed that by
correcting problems in the body's structure, through the use of manual techniques
now known as osteopathic manipulative medicine (OMM), the body's ability to
function and to heal itself could be greatly improved. He also promoted the
idea of preventive medicine and endorsed the philosophy that physicians should
focus on treating the whole patient, rather than just the disease. He became so
skilled at reducing fractures, he became known as the "lightning bone
setter". At the time, these beliefs formed the basis of a new medical
approach, osteopathic medicine. Based on this philosophy, Still founded the
first school of osteopathy -- the American School of Osteopathy (now Kirksville
College of Osteopathic Medicine) in Kirksville, Missouri in 1892.
http://en.wikipedia.org/wiki/Aponeurosis
Aponeuroses (απο,
"away" or "of", and νευρον,
"sinew") are membranes separating muscles from each other. They have
a shiny, whitish-silvery color, and are histologically
similar to tendons,
but are very sparingly supplied with blood vessels
and nerves.
When dissected, aponeuroses are papery, and peel off by sections. The primary
regions with thick aponeurosis is in the ventral
abdominal
region, the dorsal
lumbar
region, and in the palmar
region.
Axon
http://en.wikipedia.org/wiki/Axons
An axon or nerve fiber, is a long, slender
projection of a nerve cell, or neuron,
that conducts electrical
impulses away from the neuron's cell body
or soma.
http://en.wikipedia.org/wiki/Brachial_plexus
The brachial plexus
is an arrangement of nerve fibres, running from the spine, specifically from
above the fifth cervical
vertebra to underneath the first thoracic
vertebra (C5-T1). It proceeds through the neck, the axilla
(armpit region) and into the arm. The brachial plexus is responsible for
cutaneous and muscular innervation of the entire upper limb, with two
exceptions: the trapezius
muscle innervated by the spinal
accessory nerve and an area of skin near the axilla innervated by the intercostobrachialis nerve.
Therefore, lesions of the plexus can lead to severe functional impairment.
http://en.wikipedia.org/wiki/Carl_Rogers
Carl Ransom Rogers (January 8, 1902 –
February 4, 1987) was an influential American psychologist and among the
founders of the humanistic approach to psychology. Rogers is considered to be
one of the founding fathers of psychotherapy research and was honored for his
pioneering research with the Award for Distinguished Scientific Contributions
by the American Psychological Association in 1956. The Person-centered
approach, his own unique approach to understanding personality and human
relationships, found wide application in various domains such as psychotherapy
and counseling (Client-centered therapy), education (Student-centered
learning), organizations, and other group settings. For his professional work
he was bestowed the Award for Distinguished Professional Contributions to
Psychology by the APA in 1972. Towards the end of his life he was nominated for
the Nobel Peace Prize for his work with national intergroup conflict in South
Africa and Northern Ireland. In an empirical study by Haggbloom et al. (2002)
using six criteria such as citations and recognition, Rogers was found to be
the 6th most eminent psychologist of the 20th Century and among clinicians, 2nd
only to Sigmund Freud.[1]
Cardiac muscle
http://en.wikipedia.org/wiki/Cardiac_muscle
'Cardiac muscle' is a type
of involuntary striated
muscle found within the
heart. Its function is to "pump"
blood through the circulatory
system by contracting. Metabolism Cardiac muscle is adapted to be
highly resistant to fatigue: it has a large number of mitochondria enabling
continuous aerobic respiration; numerous myoglobins (oxygen storing pigment);
and a good blood supply, which provides metabolic substrate and oxygen. The
heart is so tuned to aerobic metabolism that it is unable to pump sufficiently
in ischaemic conditions. At basal
metabolic rates, about 1% of energy is derived from anaerobic metabolism. This
can increase to 10% under moderately hypoxic conditions, but under more severe
hypoxic conditions, not enough energy can be liberated by lactate production to
sustain ventricular contractions. [1] Under basal
aerobic conditions, 60% of energy comes from fat (free fatty acids and
triacylglycerides), 35% from carbohydrates, and 5% from amino acids and ketone
bodies. However, these proportions vary widely according to nutritional state.
E.g., in starvation, lactate can be recycled by the heart. There is a cost to
lactate recycling, since one NAD+ is reduced to get pyruvate from lacate, but
the pyruvate can then be burnt aerobically in the TCA cycle, liberating much
more energy. In diabetes, more fat and less carbohydrate is used, due to the
reduced induction of GLUT4
glucose transporters to the cell surfaces. However, contraction itself plays a
part in bringing GLUT4 transporters to the surface. [2] This is true of
skeletal muscle, but relevant in particular to cardiac muscle, since it is
always contracting. [edit]
Contractions [edit]
Initiation Unlike skeletal muscle, which
contracts in response to nerve
stimulation, and like single unit smooth muscle, cardiac muscle is myogenic, meaning that
it is self-excitable stimulating contraction without a requisite electrical
impulse coming from the central nervous system. A single cardiac muscle cell, if left without
input, will contract rhythmically at a steady rate; if two cardiac muscle cells
are in contact, whichever one contracts first will stimulate the other to
contract, and so on. This inherent contractile activity is heavily regulated by
the autonomic
nervous system. If synchronization of cardiac
muscle contraction is disrupted for some reason (for example, in a heart attack),
uncoordinated contraction known as fibrillation can result.
This transmission of impulses makes cardiac muscle tissue similar to nerve
tissue, although cardiac muscle cells are notably connected to each other by intercalated discs. Intercalated
discs conduct electrochemical potentials directly between the cytoplasms of
adjacent cells via gap junctions.
In contrast to the chemical synapses used by neurons,
electrical synapses, in the case of
cardiac muscle, are created by ions flowing from cell to cell, known as an
action potential.
[edit]
Intercalated disc An intercalated disc is an undulating double membrane
separating adjacent cells in cardiac muscle fibers. Intercalated discs support
synchronized contraction of cardiac tissue. They can easily be visualized by a
longitudinal section of the tissue. Three types of membrane junctions exist
within an intercalated disc—fascia adherens, macula adherens, and gap
junctions. Fascia adherens are anchoring sites for actin, and connects to the
closest sarcomere. Macula adherens stop separation during contraction by
binding intermediate filaments joining the cells together also called a
desmosome. Gap junctions allow action potentials to spread between cardiac
cells by permitting the passage of ions between cells, producing depolarization
of the heart muscle. When observing cardiac tissue through a microscope,
intercalated discs are an identifying feature of cardiac muscle[edit]
Rate Specialized pacemaker cells in the sinoatrial node normally
determine the overall rate of contractions, with an average resting pulse of 72
beats per minute. The central nervous system does not directly create the
impulses to contract the heart, but only sends signals to speed up or slow down
the heart rate through the autonomic
nervous system using two opposing kinds of
modulation: (1) sympathetic
nervous system (fight or flight response) (2) parasympathetic
nervous system (rest and repose) Since cardiac
muscle is myogenic, the pacemaker serves only to modulate and coordinate
contractions. The cardiac muscle cells would still fire in the absence of a
functioning SA node pacemaker, albeit in a chaotic and ineffective manner. This
condition is known as fibrillation.
Note that the heart can still beat properly even if its connections to the
central nervous system are completely severed. [edit]
Role of calcium In contrast to skeletal muscle, cardiac muscle
cannot contract in the absence of extracellular calcium ions as well as
extracellular potassium ions. In this sense, it is intermediate between smooth muscle, which has a
poorly developed sarcoplasmic reticulum and derives its calcium across the
sarcolemma; and skeletal muscle
which is activated by calcium stored in the sarcoplasmic
reticulum (SR). The reason for the calcium dependence is
due to the mechanism of calcium-induced
calcium release (CICR) from the SR that must occur
under normal excitation-contraction (EC) coupling to cause contraction. [edit]
Appearance [edit]
Striation Cardiac muscle exhibits cross striations formed by alternation
segments of thick and thin protein filaments which are anchored by segments
called Z-lines.
The primary structural proteins of cardiac muscle are actin
and myosin. The actin
filaments are thin causing the lighter appearance of the I bands in muscle,
while myosin is thicker and darker lending a darker appearance to the
alternating A bands in cardiac muscle as observed by a light enhanced
microscope. [edit]
Nuclei Cardiac muscle can be distinguished from skeletal muscle because
cardiac muscle nuclei are centrally located among the myofibrils, unlike the
peripheral nuclei of skeletal muscle.[3] A unique aspect
of cardiac muscle is the number of nuclei found inside the cell. Skeletal
muscle cells are multinucleated from the fusion of muscle cells, whereas smooth
muscle cells are strictly mononucleated, and cardiac muscle cells are
predominantly mononucleated in humans. In some non-human species the foetal and
post-parturition cardiac myocytes undergo a change from a mononuclear cell to a
binuclear cell. In some cases the myocytes further develop into multinucleated
cells. Amongst most species the cardiac myocyte consists of 90% binucleated
cells and 5% mono-gram and multinucleated-gram cells. The exact proportions
depend upon the species in question. [edit]
T-Tubules
Another histological difference between
cardiac muscle and skeletal muscle is that the T-tubules in cardiac
muscle are shorter, broader and run along the Z-Discs. There are fewer
T-tubules in comparison with Skeletal muscle. Additionally, cardiac muscle
forms dyads instead of the triads formed between the T-tubules and the sarcoplasmic
reticulum in skeletal muscle. [edit]
Intercalated Discs Under light microscopy, intercalated
discs appear as thin, typically dark-staining lines dividing adjacent cardiac
muscle cells. The intercalated discs run perpendicular to the direction of
muscle fibers. Under electron microscopy, an intercalated disc's path appears
more complex. At low magnification, this may appear as a convoluted electron
dense structure overlying the location of the obscured Z-line. At high
magnification, the intercalated disc's path appears even more convoluted, with
both longitudinal and transverse areas appearing in longitudinal section.[4] Gap junctions (or nexus
junctions) fascia adherens
(resembling the zonula adherens),
and desmosomes are visible. In
transverse section, the intercalated disk's appearance is labyrinthine and may
include isolated interdigitations.
http://en.wikipedia.org/wiki/Celiac_plexus
The
celiac plexus is located near where the celiac
trunk,
superior mesenteric artery, and renal
arteries
branch from the abdominal aorta. It is
behind the stomach and
the omental bursa and in
front of the crura of the diaphragm, on
the level of the first lumbar
vertebra,
L1. The plexus is formed (in part) by the greater and lesser splanchnic
nerves
of both sides, and also parts of the right vagus
nerve.
The celiac plexus proper consists of the celiac
ganglia
with a network of interconnecting fibers. The aorticorenal ganglia are
often considered to be part of the celiac ganglia, and thus, part of the
plexus. The celiac plexus is often popularly referred to as the solar plexus,
generally in the context of a blow to the stomach. In many of these cases, it
is not the celiac plexus itself being referred to, but rather the region where
it is located. A blow to the stomach can upset this region. This can cause the
diaphragm to spasm, resulting in difficulty in breathing — a sensation commonly
known as "getting the
wind knocked out of you". A blow to this region can also
affect the celiac plexus itself, possibly interfering with the functioning of
the viscera, as well as causing great pain. A celiac
plexus block by means of fluoroscopically guided
injection is sometimes used to treat intractable pain from cancers such as pancreatic
cancer.
According to Hindu
beliefs, the solar plexus chakra is "the center of etheric-psychic
intuition: a vague or non-specific, sensual sense of knowing; a vague sense of
size, shape, and intent of being."[1] As
such, some psychics recommend "listening" to it since it may help out
in making better decisions in one's life on many different levels.[2]
http://en.wikipedia.org/wiki/Cervical_plexus
The
cervical plexus is a plexus of the ventral
rami
of the first four cervical spinal nerves which
are located from C1 to C4 cervical segment in the neck. They
are located laterally to the transverse processes between prevertebral muscles
from the medial side and vertebral (m.scalenus, m.levator
scapulae,
m.splenius cervicis) from
lateral side. Here there is anastomosis with accessory
nerve,
hypoglossal nerve and sympathetic
trunk.
It
is located in the neck, deep to sternocleidomastoid.
Nerves formed from the cervical plexus innervate the back of the head, as
well as some neck muscles. The branches of the cervical plexus emerge from the posterior triangle at the
nerve point, a
point which lies midway on the posterior border of the Sternocleidomastoid.
Chemoreceptors
Detect
taste in the mouth, smell in the nose, and chemicals in body fluids, such as
oxygen, carbon dioxide, water, and glucose.
Cohort study
http://en.wikipedia.org/wiki/Cohort_study
A
cohort study is a form of longitudinal study used
in medicine and social
science.
It is one type of study design. In
medicine, it is usually undertaken to obtain evidence to try to refute the
existence of a suspected association between cause and disease; failure to
refute a hypothesis strengthens confidence in it. Crucially, the cohort is
identified before the appearance of the disease under investigation. The study
groups, so defined, are observed over a period of time to determine the
frequency of new incidence of the studied disease among them. The cohort cannot
therefore be defined as a group of people who already have the disease.
Distinguishing causality from mere correlation cannot usually be done with
results of a cohort study alone.
http://en.wikipedia.org/wiki/Connective_tissue
Connective
tissue
is one of the four types of tissue in
traditional classifications (the others being epithelial, muscle, and nervous
tissue.)
It is largely a category of exclusion rather than one with a precise
definition, but all or most tissues in this category are similarly: Involved in
structure and support. Derived from mesoderm,
usually. Characterized largely by the traits of non-living tissue.
Blood, cartilage, and bone are
usually considered connective tissue, but because they differ so substantially
from the other tissues in this class, the phrase "connective tissue
proper" is commonly used to exclude those three. There is also variation
in the classification of embryonic connective tissues; on this page they will
be treated as a third and separate category. When heated to 190 degrees
farenheit, connective tissue emits a "Vinegar Like Stench Areolar (or loose) connective
tissue
holds organs and epithelia in
place, and has a variety of proteinaceous
fibres, including collagen and elastin. It is
also important in inflammation. Adipose
tissue
contains adipocytes, used
for cushioning, thermal insulation, lubrication
(primarily in the pericardium) and energy
storage. [fat] Dense connective tissue (or,
less commonly, fibrous connective tissue) forms
ligaments and tendons. Its
densely packed collagen fibres have great tensile strength. Reticular connective tissue is a
network of reticular fibres (fine collagen, type III) that form a soft skeleton
to support the lymphoid organs
(lymph
nodes,
bone
marrow,
and spleen.) Blood
functions in transport. Its extracellular matrix is blood
plasma,
which transports dissolved nutrients, hormones, and carbon
dioxide
in the form of bicarbonate. The
main cellular component is red
blood cells.
Bone makes
up virtually the entire skeleton in adult vertebrates. Cartilage makes
up virtually the entire skeleton in chondrichthyes. In
most other vertebrates, it is
found primarily in joints, where it provides cushioning.
The extracellular matrix of cartilage is composed primarily of collagen.
http://www.bartleby.com/107/250.html
The
posterior surface (facies posterior) (Fig. 1087) is
rounded and broad behind the right lobe, but narrow on the left. Over a large
part of its extent it is not covered by peritoneum; this uncovered portion is
about 7.5 cm. broad at its widest part, and is in direct contact with the
diaphragm. It is marked off from the upper surface by the line of reflection of
the upper layer of the coronary ligament, and from the under surface by the
line of reflection of the lower layer of the coronary ligament.
Craniosacral
therapy
http://en.wikipedia.org/wiki/Craniosacral_Therapy
Cranial Technique [4] [5] [6] [7] [8] [9] [10] [11] [12]
Selected Cranial Sacral Research [13] [14] [15] [16] [17] [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] [32] [33] [34]
Craniosacral
therapy (also called CST, cranial osteopathy, also spelled CranioSacral therapy)
is a method of alternative medicine used by massage therapists, naturopaths,
chiropractors and osteopaths, who manually apply a subtle movement of the
spinal and cranial bones to bring the central nervous system into harmony. This
therapy involves assessing and addressing the movement of the cerebrospinal
fluid (CSF), which can be restricted by trauma to the body, such as through
falls, accidents, and general nervous tension. By gently working with the
spine, the skull and its cranial sutures, diaphragms, and fascia, the
restrictions of nerve passages are eased, the movement of CSF through the
spinal cord can be optimized, and misaligned bones can be restored to their
proper position. This therapy is said to be particularly useful for mental
stress, neck and back pain, migraines, TMJ Syndrome, and for chronic nervous
conditions such as fibromyalgia.[1][2][3]
Criticisms
Skeptics existing both inside and
outside the osteopathic profession level the following criticisms at
Craniosacral therapy:
Lack of evidence for the existence of
"cranial bone movement"
The scientific evidence for cranial bone
movement is insufficient to support the theories claimed by craniosacral
practitioners. Scientific research supports the theory that the cranial bones
fuse during adolescence, making movement impossible. However, this research
only points to fusion of the base of the skull which is not contested in
craniosacral therapy and does not address movement in the superior plates. As
such, this research plays no part in disproving the type of cranial bone
movement as postulated by craniosacral therapy.[37]
Lack of evidence for the existence of
the "cranial rhythm"
While evidence exists for cerebrospinal
fluid pulsation, one study states it is caused by the functioning of the
cardiovascular system and not by the workings of the craniosacral system.[38]
Lack of evidence linking "cranial
rhythm" to disease
No research to date has supported the
link between the "cranial rhythm" and general health.
Lack of evidence "cranial
rhythm" is detectable by practitioners
Operator interreliability has been very
poor in the studies that have been done. Five studies showed an operator
interreliability of zero.[39]
The one study showing some operator
interreliability has been criticized as deeply flawed in a report to the
British Columbia Office of Health Technology Assessment.[40]
Dense connective tissue
http://en.wikipedia.org/wiki/Dense_connective_tissue
Dense connective tissue,
also called dense fibrous tissue, has collagen fibers as its
main matrix element. It is mainly composed of collagent type I. Crowded between
the collagen fibers are rows of fibroblasts, fiber-forming
cells, that manufacture the fibers. Dense connective tissue forms strong,
rope-like structures such as tendons
and ligaments. Tendons attach
skeletal muscles
to bones; ligaments
connect bones to bones at joints. Ligaments are more stretchy and contain more
elastic fibers than tendons. Dense connective tissue also make up the lower
layers of the skin (dermis), where it is
arranged in sheets. [edit]
Types It is often divided into "regular" and "irregular": Dense
regular connective tissue provides strong connection between different
tissues. The collagen fibers in dense regular connective tissue are bundled in
a parallel fashion. Tendons,
which connect muscle to bone, derive their strength from the regular,
longitudinal arrangement of bundles of collagen fibers. Ligaments bind bone to
bone and are similar in structure to tendons. Dense irregular connective
tissue has fibers that are not arranged in parallel bundles as in dense
regular connective tissue. This tissue comprises a large portion of the dermal
layer of skin.
http://en.wikipedia.org/wiki/Thoracic_diaphragm
http://en.wikipedia.org/wiki/Image:Gray391.png
{kind=link}
http://www.bartleby.com/107/117.html
In the anatomy of mammals,
the diaphragm is a shelf of muscle
extending across the bottom of the ribcage. The diaphragm
separates the thoracic cavity
(with lung and heart)
from the abdominal cavity
(with digestive system
and urogenital system).
In its relaxed state, the diaphragm is shaped like a dome. It is controlled by
the phrenic nerve.
In order to avoid confusion with other types of diaphragm, it is sometimes
referred to as the thoracic diaphragm. Any reference to the
diaphragm is understood to refer to this structure. It is crucial in respiration:
in order to draw air into the lungs, the diaphragm contracts, thus enlarging
the thoracic cavity and reducing intra-thoracic pressure (the external
intercostals muscles also participate in
this enlargement). When the diaphragm relaxes, air is exhaled by elastic recoil
of the lung and the tissues lining the thoracic cavity in conjunction with the
abdominal muscle which act as the antagonist pair to diaphragm's contraction Antagonist
(muscle). The diaphragm is also found in other vertebrates such as reptiles. It is
responsible for all the breathing related to voice.
The diaphragm also helps to expel vomit,
feces, and urine
from the body by increasing intra-abdominal pressure. A hiatal hernia can result from
a tear or weakness in the diaphragm near the gastroesophageal
junction.
If the diaphragm is struck, or otherwise
spasms, breathing will
become difficult. This is called having
the wind knocked out of you.
A hiccup occurs when the
diaphragm contracts periodically without voluntary control. Diaphragmatic
injuries result from either blunt or penetrating trauma. The Diaphragm is a
dome-shaped musculofibrous septum which separates the thoracic from the
abdominal cavity, its convex upper surface forming the floor of the former, and
its concave under surface the roof of the latter. Its peripheral part consists
of muscular fibers which take origin from the circumference of the thoracic outlet and converge to
be inserted into a central tendon. The muscular fibers may be grouped according
to their origins into three parts: ORIGIN-sternal=two
fleshy slips from the back of the xiphoid process. Costal=the
inner surfaces of the cartilages and adjacent portions of the lower six ribs on
either side, interdigitating with the Transversus
abdominis. Lumbar=aponeurotic arches, named the lumbocostal
arches, and from the lumbar vertebrae by two pillars
or crura. There are two lumbocostal arches, a medial
and a lateral,
on either side. [edit]
Crura and central tendon At their origins the crura are tendinous
in structure, and blend with the anterior
longitudinal ligament of the vertebral column. The central tendon of the
diaphragm is a thin but strong aponeurosis situated near
the center of the vault formed by the muscle, but somewhat closer to the front
than to the back of the thorax,
so that the posterior muscular fibers are the longer. [edit]
Openings in the Diaphragm The diaphragm is pierced by a series of apertures
to permit of the passage of structures between the thorax and abdomen. Three
large openings—the aortic,
the esophageal, and the vena cava—and
a series of smaller ones are described. caval opening=T8=inferior vena
cava, and some branches of the right phrenic nerve. esophageal hiatus=T10=esophagus, the vagus nerves, and some small
esophageal
arteries. aortic hiatus=T12=the aorta,
the azygos vein,
and the thoracic duct.
two lesser aperture of right crus=greater
and lesser right splanchnic
nerves. three lesser aperture of left crus=greater and
lesser left splanchnic
nerves and the hemiazygos vein. behind the
diaphragm, under the medial
lumbocostal arches= gangliated trunks of the sympathetic. areolar tissue
between the sternal and costal parts (see also foramina of
Morgagni)= the superior
epigastric branch of the internal mammary
artery and some lymphatics from the
abdominal wall and convex surface of the liver.
areolar tissue between the
fibers springing from the medial and lateral
lumbocostal arches= This interval is less
constant; when this interval exists, the upper and back part of the kidney
is separated from the pleura
by areolar tissue
only. Variations
The sternal portion of the muscle is
sometimes wanting and more rarely defects occur in the lateral part of the central tendon or adjoining muscle
fibers.
Dermis
http://en.wikipedia.org/wiki/Dermis
The dermis is a layer of skin
beneath the epidermis
that consists of connective tissue
and cushions the body from stress and strain. The dermis is tightly connected
to the epidermis by a basement membrane. It also
harbors many nerve endings that provide the sense of touch and heat. It
contains the hair follicles,
sweat glands, sebaceous glands, apocrine glands
and blood vessels.
The blood vessels in the dermis provide nourishment and waste removal to its
own cells as well as the Stratum basale of the epidermis.
Dorsal root ganglion
http://en.wikipedia.org/wiki/Dorsal_root_ganglia
http://en.wikipedia.org/wiki/Image:Gray675.png
{kind=link}
In anatomy and neurology, the dorsal
root ganglion
(or spinal ganglion) is a nodule on a dorsal root that contains
cell bodies of neurons
in afferent
spinal nerves. All of the axons
in the dorsal root convey somatosensory
information, bringing sensory information into the brain
and spinal cord.
These neurons are of the pseudo-unipolar
type, meaning they have two axons, one that conveys sensory information from
the body to the soma of the neuron and one from the soma to the junction in the
dorsal horn of the spinal cord.
The dorsal root ganglia lie along the
vertebral columna by the spine.
Efferent
Conducting outward from a part or organ;
specifically: conveying nervous impulses to an effector (muscles organs).
Conveys nerve impulses from the brain and spinal cord to effectors that may be
either muscles or glands.
Epidermis (skin)
http://en.wikipedia.org/wiki/Epidermis_%28skin%29
Epidermis
is the outermost layer of the skin.
It forms the waterproof, protective wrap over the body's surface and is made up
of stratified squamous epithelium
with an underlying basal lamina.
Components The epidermis contains no blood vessels, and is
nourished by diffusion
from the dermis. The main type
of cells which make up the epidermis are keratinocytes, melanocytes, Langerhans cells and Merkels cells. [edit]
Layers The epidermis is divided into several layers where cells are formed
through mitosis at the
innermost layers. They move up the strata changing shape
and composition as they differentiate and become filled with keratin. They
eventually reach the top layer called stratum corneum and become sloughed off,
or desquamated. This process is called keratinization and takes place
within weeks. The outermost layer of epidermis consists of 25 to 30 layers of
dead cells. [edit]
Sublayers Epidermis is divided into the following 5 sublayers or strata, listed
from the superficial to deep: Stratum corneum Stratum lucidum Stratum
granulosum Stratum spinosum Stratum
germinativum (also called "stratum
basale") Mnemonics
used for remembering the layers of the skin (using "stratum basale"
instead of "stratum germinativum"): "Corn Lovers Grow
Several Bales" (from superficial to deep) "Before
Signing, Get Legal Counsel" (from deep to
superficial)
http://en.wikipedia.org/wiki/Epithelium
In biology and medicine, epithelium
is a tissue
composed of a layer of cells. Epithelium
lines both the outside (skin)
and the inside cavities and lumen of bodies. The
outermost layer of our skin
is composed of dead stratified squamous, keratinized
epithelial cells. Mucous membranes
lining the inside of the mouth, the esophagus, and part of the rectum are lined
by nonkeratinized stratified squamous epithelium. Other, open to outside body
cavities are lined by simple squamous or columnar epithelial cells. Other
epithelial cells line the insides of the lungs,
the gastrointestinal
tract, the reproductive and urinary tracts,
and make up the exocrine
and endocrine glands.
Functions of epithelial cells include secretion, absorption, protection,
transcellular transport, sensation detection, and selective permeability. Endothelium (the inner
lining of blood vessels,
the heart, and lymphatic vessels) is a
specialized form of epithelium. Another type, Mesothelium, forms the
walls of the pericardium,
pleurae, and peritoneum. In humans,
epithelium is classified as a primary body tissue, the other ones being connective tissue, muscle tissue and nervous tissue. Squamous:
Squamous cells are flat cells with an irregular flattened shape. A one-cell
layer of simple squamous epithelium forms the alveoli of the respiratory membrane,
and the endothelium
of capillaries, and is a minimal barrier to diffusion. Other places
where squamous cells can be found include the filtration tubules of the kidneys, and the major
cavities of the body. These cells are relatively inactive metabolically, and
are associated with the diffusion of water, electrolytes, and other
substances. Cuboidal: As the name suggests, these cells have a shape
similar to a cube, meaning its width is the same size as its height. The nuclei of these cells
are usually located in the center. Columnar: These cells are taller than
they are wide. Simple columnar epithelium is made up of a single layer of cells
that are longer than they are wide. The nucleus is also closer to the base of
the cell. The small intestine
is a tubular organ
lined with this type of tissue. Unicellular glands called goblet cells are
scattered throughout the simple columnar epithelial cells and secrete mucus.
The free surface of the columnar cell has tiny hairlike projections called microvilli. They increase
the surface area for absorption. Transitional: This is a specialized
type of epithelium found lining organs that can stretch, such as the urothelium that lines the
bladder and ureter of mammals.
Since the cells can slide over each other, the appearance of this epithelium
depends on whether the organ is distended or contracted: if distended, it
appears as if there are only a few layers; when contracted, it appears as if
there are several layers.
Esophagus
http://en.wikipedia.org/wiki/Esophagus
http://www.bartleby.com/107/245.html
http://education.yahoo.com/reference/gray/illustrations/figure;_ylt=A86.OK3vFLZGkzsBH3dtHokC?id=1032
http://en.wikipedia.org/wiki/Image:Gray1134.png
{kind=link}
The esophagus (Fig. 1032) or gullet is a
muscular canal, about 23 to 25 cm. long, extending from the pharynx to the
stomach. It begins in the neck at the lower border of the cricoid cartilage,
opposite the sixth cervical vertebra, descends along the front of the vertebral
column, through the superior and posterior mediastina, passes through the
diaphragm, and, entering the abdomen, ends at the cardiac orifice of the
stomach, opposite the eleventh thoracic vertebra.
Exteroceptors
Provide information about the external
environment. They are sensitive to stimuli outside the body and transmit
sensations of hearing, sight, smell, taste, touch, pressure, temperature, and
pain. Exteroceptors are located at or near the surface of the body.
http://www.bartleby.com/107/250.html
http://www.bartleby.com/107/illus1085.html
(This demonstrates the falciform lig superior attachment to the diaphragm.
The superior surface is attached to the
diaphragm and anterior abdominal wall by a triangular or falciform fold of
peritoneum, the falciform ligament, in the free margin of which is a rounded
cord, the ligamentum teres (obliterated umbilical vein). The line of attachment
of the falciform ligament divides the liver into two parts, termed the right
and left lobes, the right being much the larger.
http://en.wikipedia.org/wiki/Ganglion
In anatomy, a ganglion
(pl. ganglia) is a tissue mass, which is
composed mainly of somata and dendritic structures,
which often interconnect with each other to form a complex system of ganglia
known as a plexus. These
structures provide relay points and intermediary connections between different neurological
structures in the body, such as the peripheral
and central
nervous systems.
There are two major groups of ganglia: dorsal root
ganglia (also known as the spinal ganglia) and autonomic
ganglia. The former contains the cell bodies of
sensory (afferent)
nerves and the latter
contains the cell bodies of autonomic
nerves. In the autonomic
nervous system, fibers from the central nervous
system to the ganglion are known as preganglionic
fibers, while those from the ganglion to the
effector organ are called postganglionic fibers.
Gastroesophageal Reflux Disease (GERD)
http://en.wikipedia.org/wiki/Gastroesophageal_reflux_disease
Gastroesophageal Reflux Disease
(GERD; or GORD when spelling œsophageal, the BrE form) is defined as
chronic symptoms or mucosal
damage produced by the abnormal reflux of gastric contents into the esophagus[1]. This is
commonly due to transient or permanent changes in the barrier between the
esophagus and the stomach.
This can be due to incompetence of the lower esophageal
sphincter (LES), transient LES relaxation,
impaired expulsion of gastric reflux from the esophagus, or a hiatal hernia. Adults Heartburn is the major
symptom of acid in the esophagus, characterized by burning discomfort behind
the breastbone (sternum).
Findings in GERD include esophagitis
(reflux esophagitis) — inflammatory changes in the
esophageal lining (mucosa) — strictures, difficulty
swallowing (dysphagia),
and chronic chest pain.
Patients may have only one of those findings. Typical GERD symptoms include
cough, hoarseness, voice changes, chronic ear ache, burning chest pains, nausea
or sinusitis. GERD
complications include stricture formation, Barrett's
esophagus, esophageal ulcers,
and possibly even lead to esophageal cancer, especially in
adults over 60 years old. Occasional heartburn is common but does not
necessarily mean one has GERD. Patients with heartburn symptoms more than once
a week are at risk of developing GERD. A hiatal hernia is usually asymptomatic, but the
presence of a hiatal hernia is a risk factor for developing GERD.[edit]
Generator Potential
Generator Potentials differ from nerve
action potentials in several ways. A generator potential is a localized
response that decreases in intensity as it travels along a nerve fiber, whereas
a nerve action potential is propagated at a constant and maximum strength. A
generator potential is a graded response, that is within limits, the stronger
and more frequent the stimulus, the greater the magnitude of the generator
potential. A nerve action potential obeys the all-or-none principal. A
generator potential usually lasts longer than 1 to 2 msec, a nerve action
potential does not. A generator potential does not have a refractory period,
whereas a nerve action potential has one that lasts for about 1 msec. This
means that if a second stimulus is
applied to a receptor before a generator potential resulting from the first
stimulus disappears, the second stimulus can add to the effect of the first,
producing an even greater generator potential. Hus, summation in producting
generator potentials is possible, but summation of nerve action potentials is
not. The generator potential only travels a few millimeters before dying out.
When a generator potential reashes threshold, it initiates a nerve action
potential. The function of a generator potential is to convert a stimulus into
a nerve action potential.
Golgi tendon organ
http://en.wikipedia.org/wiki/Golgi_tendon_organs
http://en.wikipedia.org/wiki/Image:Gray938.png
{kind=link}
http://www.anatomyfacts.com/Research/golgi.bmp
{kind=link}
The Golgi organ (also called Golgi
tendon organ, neurotendinous organ or neurotendinous spindle), is a proprioceptive sensory receptor organ that is
located at the insertion of skeletal muscle fibres into the tendons
of skeletal muscle.
The Golgi organ should not be confused with the Golgi Apparatus, which is an
organelle in the eukaryotic cell,
or the Golgi stain,
which is an histologic
stain for neuron cell bodies. Anatomy The
body of the organ is made up of strands of collagen that are
connected at one end to the muscle fibers and at the other merge into the
tendon proper. Each tendon organ is innervated by a single type Ib sensory
afferent fiber that branches and terminates as
spiral endings around the collagen strands. The Ib afferent axon is a large
diameter, myelinated axon. Each
neurotendinous spindle is enclosed in a fibrous capsule which contains
a number of enlarged tendon fasciculi (intrafusal fasciculi). One or more nerve
fibres perforate the side of the capsule and lose their medullary sheaths; the
axis-cylinders subdivide and end between the tendon fibers in irregular disks
or varicosities (see figure). [edit]
Function During muscle contraction the strands of collagen are stretched as the
muscle shortens. This stretching deforms the terminals of the Ib afferent axon,
opening stretch-sensitive cation
channels. As a result, the axon is depolarized and fires nerve impulses up to the central nervous
system via the spinal cord. The action
potential frequency signals the force
being developed within the muscle. This sensory feedback plays an
important role in spinal reflexes
and in the central control of muscle contraction. Specifically, it is
postulated that because a Golgi tendon organ exists in serial connection with
muscle fibers, it can measure the tension that each muscle contraction builds
up. The Ib afferent axon synapses
with interneurons
within the spinal cord and also relays information to the brain. One of the main
spinal reflexes receiving an input from the Ib afferent is the autogenic inhibition reflex,
which is involved with the regulation of the force profile of on-going muscle
contractions.
The ascending or afferent pathways to the
cerebellum are the dorsal
and ventral spinocerebellar
tracts and are involved in the cerebellar regulation
of movement. [edit]
History It was once believed that Golgi tendon organs were responsible
for the clasp-knife
reflex observed in spinal cord-injured
patients. This theory has been rejected in favor of one that explains the
reflex with free nerve
endings.
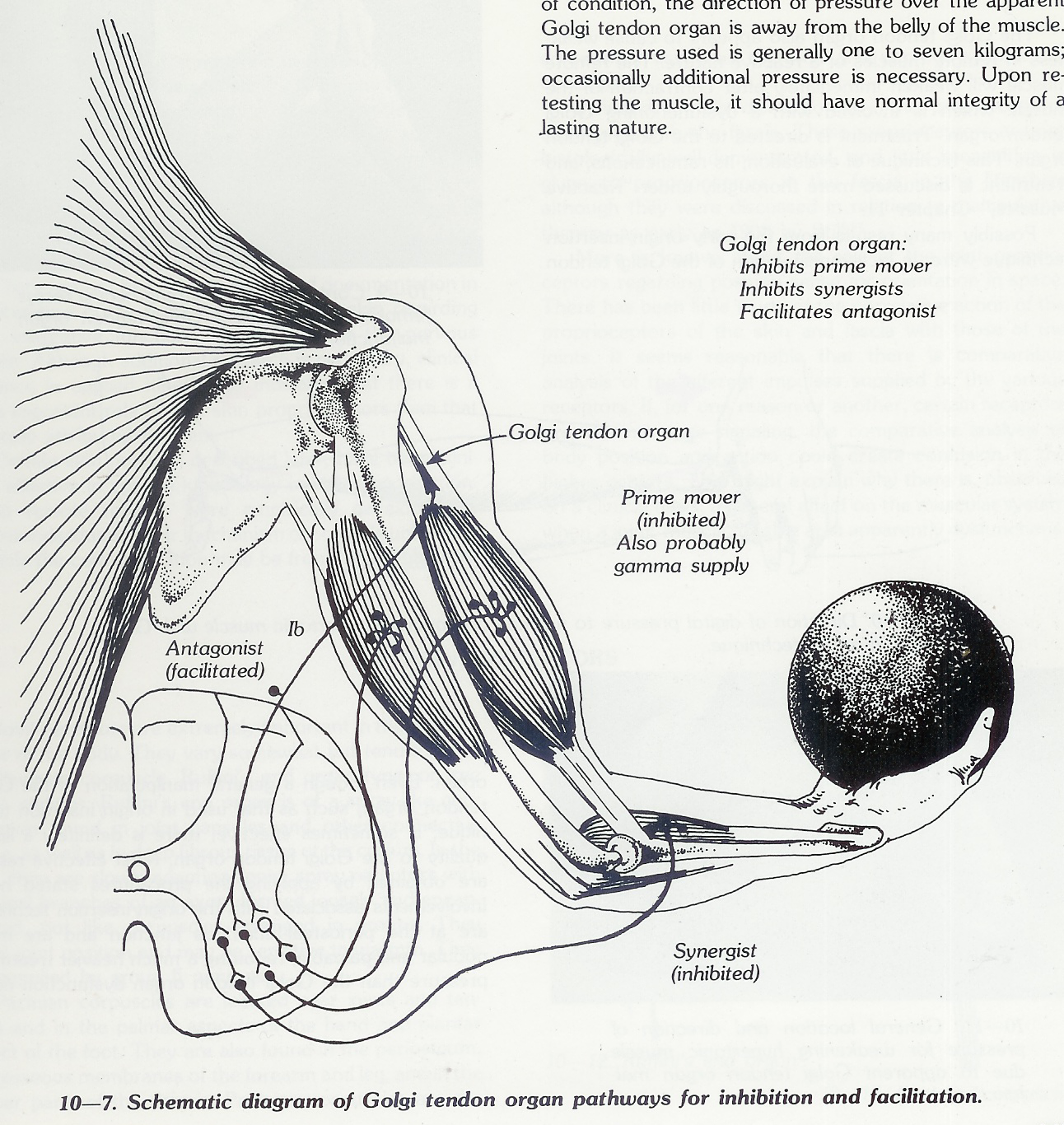
The Golgi tendon organs are located in
the tendon close to the musculotendinous junction. A few to many muscle fibers
are attached to each Golgi tendon organ, with an average of 10-15. The Golgi
tendon organ is ituated in series with
the muscle, whereas the neuromuscular spindle is parallel to the muscle. The
neuromuscular spindle monitors the length of the muscle, while the Golgi tendon
organ monitors the tension of the muscle. Stimulation of the Golgi tendon organ
is from contraction of the muscle, with stronger stimulation from greater
contraction. The Golgi tendon organ inhibits the muscle with which it is
associated. The tendon receptors have afferent nerve supply of the large group
I. The neuron is similar to the group I afferent of the neuromuscular spindle
and is differentiated as being Ib, while the neuromuscular spindle nerve is la.
Transmission from the Golgi tendon organ goes to both local areas in the cord
and through the spinal cerebellar tracks into the cerebellum. The local signal
excites interneurons which in turn inhibit the anterior alpha motor neuron of
its own muscle and synergists, while facilitating antagonists. The inhibitory
nature of the Golgi tendon organ acts as a protective mechanism for the muscle.
Many muscles have much greater strength potential than the structure can withstand.
A failure of muscle control can cause possible avulsion or tearing of the
muscle itself. Stimulation to the Golgi tendon’ organ inhibits the muscle from
going past its structural capabilities. An example of the effectiveness of the
Golgi tendon apparatus is observing individuals arm-wrestling. The loser
generally gives out completely - all at once - when impulses from the Golgi
tendon organ overpower the alpha motor neuron impulses and shut the muscle
down. It is observed, however, that many trained weight-lifters apparently have
learned to mentally override the Golgi tendon mechanism to provide a greater
amount of strength potential. This can, of course, be structurally damaging to
the body, as in the situation when an arm wrestler fractures the humerus.
There is evidence that the Golgi tendon
organ, like the muscle spindle cell, can dysfunction, giving improper
communication to the cord level and higher centers. This can cause the muscle
with which it is directly associated to be either hypotonic or hypertonic, or
to possibly influence other remote muscles. .As on the neuromuscular spindle
cell, the influence of manual manipulation of the Golgi tendon can be observed
by influencing normally functioning Golgi tendon organs. The only difficulty in
performing this experiment is in applying the manipulative force at the correct
location. It requires excellent palpatory skills to find where the Golgi tendon
organ is probably located, and a certain amount of luck that the receptor is
actually there. This is necessary because a normal Golgi tendon organ will not
therapy localize, revealing its location. To cause a strong muscle to weaken in
a normal subject, digital pressure is applied over the probable location of the
Golgi tendon organ in alignment with the muscle fibers away from the belly of
the muscle. If the attempt is successful, there will be an immediate dramatic
weakening of the muscle which will last from approximately a half-minute to
several minutes. In attempting this experiment, a muscle should be selected
which does not have an extensive amount of tendon surface area, and the muscle
should have adequate strength so that it is not easily overpowered. A good
muscle to use is the rectus femoris of the quadriceps group. The entire
quadriceps group is more difficult for. achieving successful weakening because
of the large area of origin of the muscles.
Homeopathy
http://en.wikipedia.org/wiki/Homeopathy
Homeopathy
(also homœopathy or homoeopathy; from the Greek,
ὅμοιος,
hómoios, "similar" + πάθος,
páthos, "suffering" or "disease") is a controversial
form of alternative
medicine that aims to treat "like with
like". Substances that cause symptoms similar to the disease in large
quantities are heavily diluted, with shaking at each stage of the dilution.
Homeopaths contend that the shaking causes some imprint (or memory) of the diluted
substance, despite the fact that at many common homeopathic dilutions, no
molecules of the original substance are likely to remain.[1] Homeopathy is
based on a vitalist
world view, which sees the underlying causes of sickness as imbalances in a
hypothetical vital force.
Proponents claim that homeopathic treatment can harmonize and re-balance the
vital force in the body, so restoring health. This claim is unsupported by
modern biology or medicine.[2][3][4][5][6] Homeopathy
traces its origins to the late 18th century when it was founded by German physician Samuel Hahnemann, who noted some
similarity of the symptoms of undiluted cinchona bark in healthy individuals
with those of malaria,
which it is used to treat. Hahnemann decided that an effective drug must produce
the symptoms in healthy individuals that are similar to the symptoms of the
sick patient which they are supposed to be treating.[7] Based on later
experiments, Hahnemann reasoned that using natural doses of substances would
generally not help patients because, if they produced effects similar to those
of the disease, they would only make symptoms worse, and thus proposed the dilution of substances
in water or alcohol,
with shaking (known as "succussion") after each dilution, in order to
try and imprint the liquid with the memory of the original substance. To
account for homeopathic remedies sometimes failing to produce lasting cures of
long-standing chronic diseases, Hahnemann proposed that the vital force in the
body has the ability to react or adapt to disturbances, referred to as the
"law of susceptibility", and that various causes can attract
hypothetical disease-causing entities called "miasms", which he
claimed could produce symptoms of disease within the body, and formed a deeper,
harder to treat cause of illness.[7] The medical
efficacy of homeopathic treatments is unconfirmed by scientific and clinical studies.[8][9][10] The hypothesis
that extreme dilution makes any drug more powerful is
antithetical to the principles of chemistry and physics as well as the
observed dose-response
relationships of conventional medicines. The scientific
community asserts there is no scientific evidence
supporting the contention that water or alcohol retain any memory of a
substance. Researchers conclude that any positive effects of homeopathic
treatment are simply a placebo effect.[6][11][8][9] Homeopaths are
also often accused of giving 'false hope' to patients who might be better
advised to seek effective conventional treatments. Studies have shown
homeopaths frequently advise patients to avoid standard medical procedures
including drugs which can prevent diseases such as malaria.[12][13] The
meta-analyses that have been done on homeopathy have confirmed that its effects
are unlikely to be beyond that of placebo, and those studies that have shown
positive results for homeopathic treatments were flawed in design. These
findings, along with the proscription by homeopaths against conventional
medicine and their encouragement of a "holistic" approach to health,
are in keeping with the conclusion of many scientists that homeopathy is a sort
of quackery.[14][15][16]
http://en.wikipedia.org/wiki/Humanism
Humanism[1][2] is a broad category of
ethical philosophies that affirm the dignity and worth of all people, based on
the ability to determine right and wrong by appeal to universal human
qualities—particularly rationality. It is a component of a variety of more
specific philosophical systems, and is incorporated into several religious
schools of thought. Humanism entails a commitment to the search for truth and
morality through human means in support of human interests. In focusing on the
capacity for self-determination, Humanism rejects the validity of
transcendental justifications, such as a dependence on faith, the supernatural,
or allegedly divinely revealed texts. Humanists endorse universal morality
based on the commonality of the human condition, suggesting that solutions to
human social and cultural problems cannot be parochial.[3]
http://en.wikipedia.org/wiki/Inferior_vena_cava
http://en.wikipedia.org/wiki/Image:Gray577.png
{kind=link}
http://en.wikipedia.org/wiki/Image:Diagram_of_the_human_heart_%28cropped%29.svg
{kind=link}
The inferior vena cava (or IVC)
is the large vein that carries de-oxygenated
blood from the lower
half of the body into the heart.
It is posterior to the
abdominal cavity and runs along side of the vertebral column on its right
side (i.e. it is a retroperitoneal
structure). It enters the right atrium at the lower
right, back side of the heart. The IVC is formed by the joining of the left and
right common iliac veins
and brings blood into the right atrium of the heart.
It also anastomoses
with the azygos vein
system (which runs on the right side of the vertebral column) and the venous plexuses
next to the spinal cord.
Because the IVC is not centrally located, there are some asymmetries in
drainage patterns. The gonadal veins and suprarenal veins drain into the
IVC on the right side, but into the renal vein on the left
side, which in turn drains into the IVC. By contrast, all the lumbar veins and hepatic veins usually drain
directly into the IVC. Note that the vein that carries de-oxygenated blood from
the upper half of the body is the superior vena
cava.
Inference
The act of passing from one proposition,
statement, or judgment considered as true to another whose truth is believed to
follow from that of the former. the act of passing from statistical sample data
to generalizations (as of the value of population parameters) usually with
calculated degrees of certainty.
Lateral arcuate ligament
http://en.wikipedia.org/wiki/Lateral_arcuate_ligament
The lateral arcuate ligament
(also lateral lumbocostal arch) is a ligament under the diaphragm
that arches across the upper part of the quadratus
lumborum. [edit]
Structure The lateral arcuate ligament runs from the front of the transverse
process of the first lumbar vertebra, and,
laterally, to the tip and lower margin of the twelfth rib.
It forms an arch over the quadratus
lumborum muscle. [edit]
See also Medial arcuate
ligament Median arcuate
ligament
http://en.wikipedia.org/wiki/Life_coach
Life coaching
is a practice of assisting clients to determine and achieve personal goals. A
coach will use a variety of methods, tailored to the client, to move through
the process of setting and reaching goals. Coaching is not targeted at
psychological illness, and coaches are not therapists
(although therapists may become coaches). [edit]
Origins and History With roots in executive
coaching, which itself drew on techniques
developed in management
consulting and leadership
training, life coaching also draws from a wide
range of disciplines, including sociology, psychology, postive adult
development, career counseling,
mentoring, and numerous
other types of counseling.
The coach applies
mentoring, values assessment,
behavior
modification, behavior modeling,
goal-setting, and other
techniques in assisting clients. Coaches are to be distinguished from
counselors, whether counselors in psychotherapy or other
careers. Writing for the International Journal of Coaching in Organizations,
Patrick Williams states: It is helpful to understand that both coaching and
therapy have the same roots. Coaching evolved from three main streams that have
flowed together: 1. The helping professions such as psychotherapy and
counseling. 2. Business consulting and
organizational development. 3. Personal
development training, such as EST,
Landmark Education,
Tony Robbins, Stephen Covey seminars, Eric Edmeades, and others. [1] Williams
further states that the movement towards Client-centered
therapy in the 1940s and 1950s by psychologists
Carl Rogers and Abraham Maslow helped shift
the emphasis in therapy towards the client becoming an active agent in their
progress and growth. He credits Maslow's 1968 treatise “Toward
a Psychology of Being” with providing the
framework for modern life coaching as it is practiced today.
Longitudinal study
http://en.wikipedia.org/wiki/Longitudinal_study
A longitudinal study is a correlational research study
that involves repeated observations of the same items over long periods of
time, often many decades. Longitudinal studies are often used in psychology to
study developmental trends across the life span. The reason for this is that
unlike cross-sectional
studies, longitudinal studies track the same
people, and therefore the differences observed in those people are less likely
to be the result of cultural differences across generations. Longitudinal
studies are also used in medicine to uncover predictors of certain diseases.
http://en.wikipedia.org/wiki/Mechanoreceptor
Detect mechanical deformation of
the receptor itself or in adjacent cells. Stimuli so detected include those
related to touch, pressure, vibration, Proprioception, hearing, equilibrium and
blood pressure. A mechanoreceptor is a sensory receptor that responds
to mechanical pressure or distortion. There are four main types in the glabrous skin of humans: Pacinian
corpuscles, Meissner's
corpuscles, Merkel's discs,
and Ruffini
corpuscles. There are also mechanoreceptors in the
hairy skin, and the hair cells in the cochlea are the most sensitive
mechanoreceptors in tranducing air pressure waves into sound. Mechanism of
sensation Mechanoreceptors are primary neurons that respond to mechanical
stimuli by firing action potentials. Peripheral transduction is believed to
occur in the end-organs. In sensory
transduction, the afferent neurons transmit the
message through a synapse
in the dorsal column
nuclei, where another neuron sends the signal
to the thalamus, where another
neuron sends the signal to the somatosensory
cortex. [edit]
Feedback More recent work has expanded the role of the mechanoreceptors for
feedback in fine motor control. Single action potentials from RAI and PC
afferents are directly linked to activation of related hand muscles,[1] whereas SAI
activation does not trigger muscle activity. [edit]
History The human work stemmed from Vallbo and Johansson's percutaneous
recordings from human volunteers in the late 1970s. Work in rhesus monkeys has
found virtually identical mechanoreceptors with the exception of Ruffini
corpuscles which are not found in the monkey. [edit]
Types There are two ways to categorize mechanoreceptors; by what kind of
sensation they perceive and by the rate of adaption. [edit]
By sensation Cutaneous mechanoreceptors provide the senses of touch,
pressure, vibration, proprioception and others. The
SAI type mechanoreceptor, with the Merkel cell end-organ, underlies the
perception of form and roughness on the skin.[2] The RAI type mechanoreceptor underlies
the perception of flutter,[3] and slip on the
skin.[4] Pacinian
receptors underlie the perception of high frequency vibration.[5] SAII
mechanoreceptors respond to skin stretch, but have not been closely linked to
either proprioceptive or mechanoreceptive roles in perception.[6]
[edit]
By rate of adaption Mechanoreceptors can also be separated into categories
based on their rates of adaptivity. When a mechanoreceptor receives a stimulus
it begins to fire impulses or action potentials at an elevated
frequency (the stronger the stimulus the higher the frequency). The cell,
however, will soon “adapt” to a constant or static stimulus and the pulses will
subside to a normal rate. Receptors that adapt quickly (i.e. quickly return to
a normal pulse rate) are referred to as ‘’phasic’’. Those receptors that are
slow to return to their normal firing rate are called ‘’tonic’’. Phasic
mechanoreceptors are useful in sensing such things as texture, vibrations, etc;
whereas tonic receptors are useful for temperature and proprioception among others.
Slowly adapting type I mechanoreceptors have multiple Merkel corpuscle
end-organs. Slowly adapting type II
mechanoreceptors have single Ruffini
corpuscle end-organs. Rapidly adapting type
I mechanoreceptors have multiple Meissner
corpuscle end-organs. Rapidly adapting type
II mechanoreceptors (usually called Pacinian) have single Pacinian
corpuscle end-organs. [edit]
Receptive field Cutaneous mechanoreceptors with small, accurate receptive fields are found in
areas needing accurate taction (e.g. the fingertips). In the fingertips and
lips, innervation density of slowly adapting type 1 and rapidly adapting type 1
mechanoreceptors are greatly increased. These two types of mechanoreceptors
have small discrete receptive fields and are thought to underly most low
threshold use of the fingers in assessing texture, surface slip, and flutter.
Mechanoreceptors found in areas of the body with less tactile acuity tend to
have larger receptive fields.
Medial arcuate ligament
http://en.wikipedia.org/wiki/Medial_arcuate_ligament
The medial arcuate ligament
(also medial lumbocostal arch) is tendinous fascia that arches over the psoas major muscle as it
passes through the diaphragm.
[edit]
Structure The medial arcuate ligament is an arch in the fascia covering the
upper part of the psoas major.
It is attached to the side of the body of the first or second lumbar vertebra; laterally, it
is fixed to the front of the transverse process of the first and, sometimes
also, to that of the second lumbar vertebra. It lies between the lateral arcuate
ligament and the midline median arcuate
ligament. [edit]
See also Lateral arcuate
ligament Median arcuate
ligament
Median arcuate ligament
http://en.wikipedia.org/wiki/Median_arcuate_ligament
The median arcuate ligament
is a ligament under the diaphragm
that connects the right and left crura of diaphragm.
[edit]
Structure The median arcuate ligament is formed by the right and left crura of
the diaphragm.
The crura connect to form an arch, behind which is the aortic hiatus. [edit]
See also Medial arcuate
ligament Lateral arcuate
ligament
Mediastinal pleura
http://en.wikipedia.org/wiki/Mediastinal_pleura
http://en.wikipedia.org/wiki/Image:Gray968.png
{kind=link}
Different portions of the parietal pleura have received
special names which indicate their position: thus, that portion which lines the
inner surfaces of the ribs and Intercostales is the costal pleura; that clothing
the convex surface of the diaphragm is the diaphragmatic
pleura; that which rises into the neck, over
the summit of the lung, is the cupula of the
pleura (cervical pleura); and that
which is applied to the other thoracic viscera is the mediastinal
pleura.
http://en.wikipedia.org/wiki/Mediastinum
The mediastinum is a
non-delineated group of structures in the thorax
(chest), surrounded by loose connective
tissue. It is the central compartment of the thoracic cavity. It contains
the heart, the great vessels of the heart, esophagus, trachea, thymus, and
lymph nodes of the central chest. The mediastinum lies between the right and
left pleuræ in and near the
median sagittal plane of the
chest. It extends from the sternum in front to the vertebral column behind, and
contains all the thoracic viscera except the lungs.
It may be divided for purposes of description into two parts: an upper portion,
above the upper level of the pericardium, which is named the superior mediastinum;
and a lower portion, below the upper level of the pericardium. This lower
portion is again subdivided into three parts, viz.: that in front of the
pericardium, the anterior
mediastinum; that containing the pericardium
and its contents, the middle
mediastinum; and that behind the pericardium,
the posterior
mediastinum. It is surrounded by the chest
wall anteriorly, the lungs laterally and the spine posteriorly. It is
continuous with the loose connective tissue of the neck,
and extends inferiorly onto the diaphragm.
Note that clinical radiologists and anatomists categorize the mediastinum in
slightly different ways. [edit]
Role in disease Main article: mediastinal tumor
The mediastinum frequently is the site
of involvement of various tumors. Mediastinitis is inflammation of the tissues
in the mediastinum, usually bacterial and due to
rupture of organs in the mediastinum. As the infection can progress very
quickly, this is a serious condition. Pneumomediastinum is the presence
of air in the mediastinum, which can lead to pneumothorax, pneumoperitoneum, and pneumopericardium
if left untreated in some cases. However, that does not always happen and
sometimes those conditions actually are the cause, not the result, of
pneumomediastinum. These two conditions frequently accompany Boerhaave's
syndrome, or spontaneous esophageal rupture.
Membrane potential
http://en.wikipedia.org/wiki/Membrane_potential
Membrane potential
(or transmembrane potential or transmembrane potential difference
or transmembrane potential gradient), is the electrical
potential difference (voltage) across a cell's plasma membrane. The plasma
membrane bounds the cell to provide a stable environment for biological
processes. Membrane potential arises from the action of ion transporters embedded in the
membrane which maintain viable ion
concentrations inside the cell. The term "membrane potential" is
sometimes used interchangeably with cell potential but is applicable to any lipid bilayer or membrane. The membrane
potential of most cells is kept relatively stable. Unlike most cells, neurons
are specialized to use changes in membrane potential for fast communication,
primarily with other neurons. When a neuron fires, the action potential travels down
the axon to the synapses: the magnitude
of the axonal membrane potential varies dynamically along its length. On
reaching a (chemical) synapse, a neurotransmitter is released
causing a localized change in potential in the membrane of the target neuron by
opening ion channels
in its membrane.
Meninges
http://en.wikipedia.org/wiki/Meninges
The
meninges (singular meninx) is the system of membranes which envelop the central
nervous system. The meninges consist of three layers: the dura mater, the
arachnoid mater, and the pia mater. The primary function of the meninges and of
the cerebrospinal fluid is to protect the central nervous system.
Mesentery
http://en.wikipedia.org/wiki/Mesentery
Mesentery is, in anatomy,
the double layer of peritoneum that connects a part of the small intestine to the posterior wall of the abdomen.
Its meaning, however, is frequently extended to include double layers of
peritoneum connecting various components of the abdominal cavity.
http://en.wikipedia.org/wiki/Mesothelium
The mesothelium
is a membrane that forms the lining of several body cavities: the pleura (thoracal cavity), peritoneum
(abdominal cavity) and pericardium (heart sac). Mesothelial tissue
also surrounds the male internal reproductive organs (the tunica vaginalis
testis) and
covers the internal reproductive organs of women (the tunica serosa uteri). Mesothelium that covers the
internal organs is called visceral mesothelium, while the layer
that covers the body walls is called the parietal
mesothelium. Mesothelium derives from the embryonic mesoderm
cell layer, that lines the coelom
(body cavity) in the embryo. It develops into the layer of cells that covers
and protects most of the internal organs of the body. The mesothelium forms a
monolayer of flattened squamous-like epithelial
cells resting on a thin basement membrane supported by connective tissue. Cuboidal
mesothelial cells may be found at areas of injury, the milky spots of the omentum,
and the peritoneal side of the diaphragm
overlaying the lymphatic lacunae.
The luminal surface is covered with microvilli.
The proteins and serosal fluid trapped by the microvilli provide a frictionless
surface for internal organs to slide past one another. The mesothelium is
composed of an extensive monolayer of specialized cells (mesothelial cells)
that line the body's serous cavities (cavities formed by a Serous membrane) and internal organs. The main
purpose of these cells is to produce a lubricating fluid that is released
between layers, providing a slippery, non-adhesive and protective surface to
facilitate intracoelomic movement. The mesothelium is also implicated in the
transport and movement of fluid and particulate matter across the serosal
cavities, leucocyte migration in response to
inflammatory mediators, synthesis of pro-inflammatory cytokines,
growth factors and extracellular
matrix proteins
to aid in serosal repair, and the release of factors to promote the disposition
and clearance of fibrin (such as plasminogen).
It is an antigen
presenting cell.
Furthermore, the secretion of glycosaminoglycans and lubricants may protect the
body against infection and tumor dissemination.
http://en.wikipedia.org/wiki/Metaphysics
a division of philosophy that is
concerned with the fundamental nature of reality and being and that includes
ontology, cosmology, and often epistemology abstract philosophical studies : a
study of what is outside objective experience. Metaphysics is the branch of
philosophy concerned with explaining the ultimate nature of reality, being, and
the world. Its name derives from the Greek words μετά
(metá) (meaning "after") and φυσικά
(physiká) (meaning "after talking about physics"),
"physics" referring to those works on matter by Aristotle in
antiquity.[2] Many philosophers such as Immanuel Kant would later argue that
certain questions concerning metaphysics (notably those surrounding the
existence of God, soul and freedom) are inherent to human nature and have
always intrigued mankind.
Metaphysics
is the branch of philosophy
that investigates principles of reality transcending those of any particular
science, traditionally including cosmology and ontology. It is also
concerned with explaining the ultimate nature of being
and the world.[1] Its name derives
from the Greek
words μετά (metá) (meaning "after") and φυσικά
(physiká) (meaning "after talking about physics"),
"physics" referring to those works on matter by Aristotle in antiquity.[2] In english,
though, "meta" means "beyond;over;transcending". Therefore,
metaphysics is the study of that which transcends physics. Many philosophers
such as Immanuel Kant
would later argue that certain questions concerning metaphysics (notably those
surrounding the existence of God,
soul and freedom) are inherent
to human nature and have always intrigued mankind. Some examples are: What is
the nature of reality?
Why does the world exist, and what
is its origin or source of creation? Does the world exist outside the mind? If
things exist, what is their objective nature? A central branch of metaphysics
is ontology, the
investigation into what types of things there are in
the world and what relations these things bear to one another. The
metaphysician also attempts to clarify the notions by which people understand
the world, including existence,
objecthood,
property,
space, time,
causality, and possibility. More recently,
the term "metaphysics" has also been used more loosely to refer to
"subjects that are beyond the physical world". A "metaphysical
bookstore", for instance, is not one that sells books on ontology, but
rather one that sells books on spirits,
faith healing,
crystal power,
occultism, and other such
topics. Before the development of modern science, scientific
questions were addressed as a part of metaphysics known as "natural
philosophy"; the term "science"
itself meant "knowledge". The Scientific
Revolution, however, made natural philosophy an empirical and experimental activity unlike
the rest of philosophy, and by the end of the eighteenth century it had begun to
be called "science" in order to distinguish it from philosophy.
Metaphysics therefore became the philosophical enquiry into subjects beyond the
physical world. Natural philosophy and science may still be considered topics
of metaphysics, if the definition of "metaphysics" includes empirical
explanations.
http://en.wikipedia.org/wiki/Muscle_spindle
http://www.anatomyfacts.com/Research/spindle1.bmp
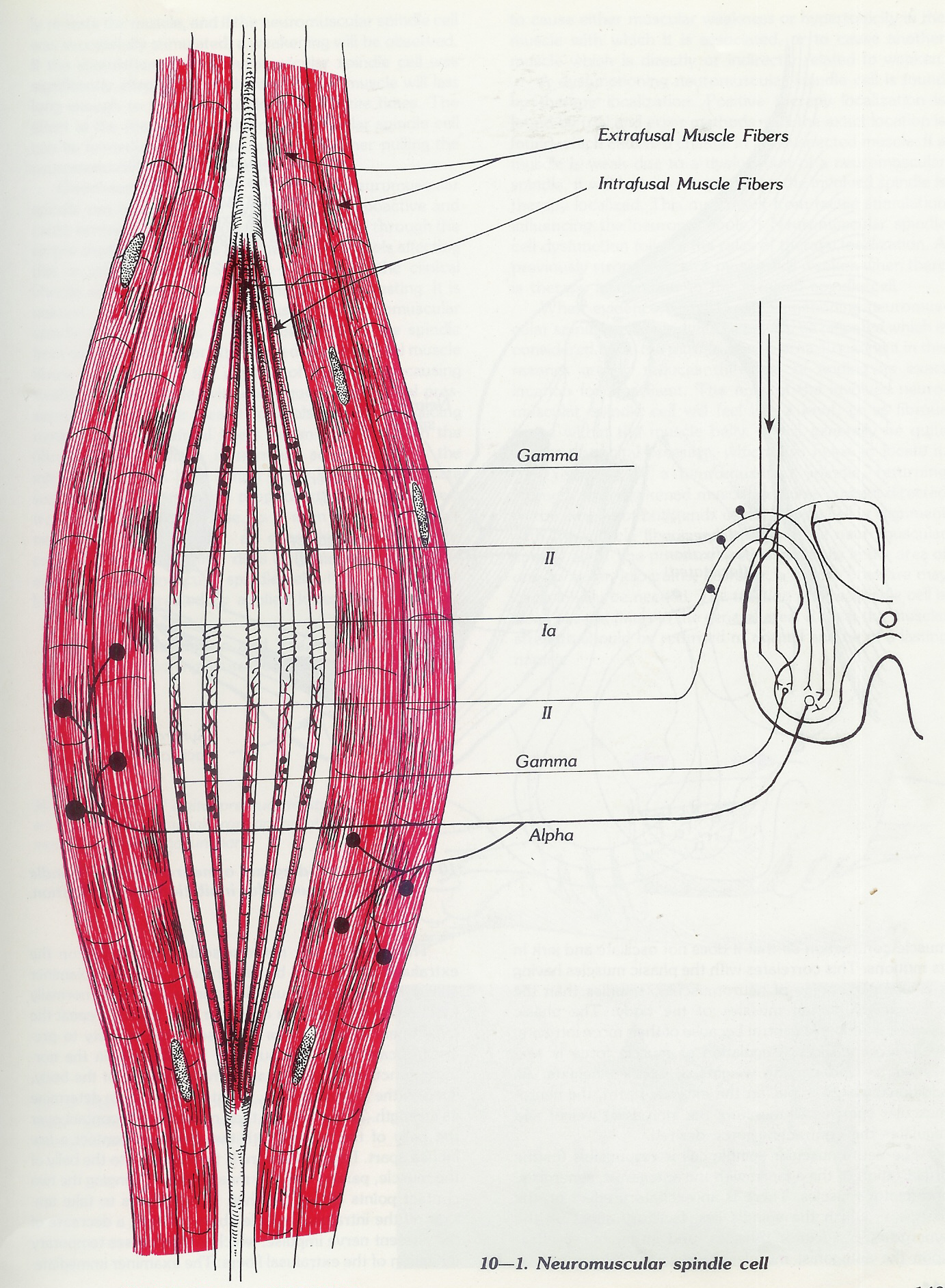{kind=link}
http://www.anatomyfacts.com/Research/spindle2.bmp
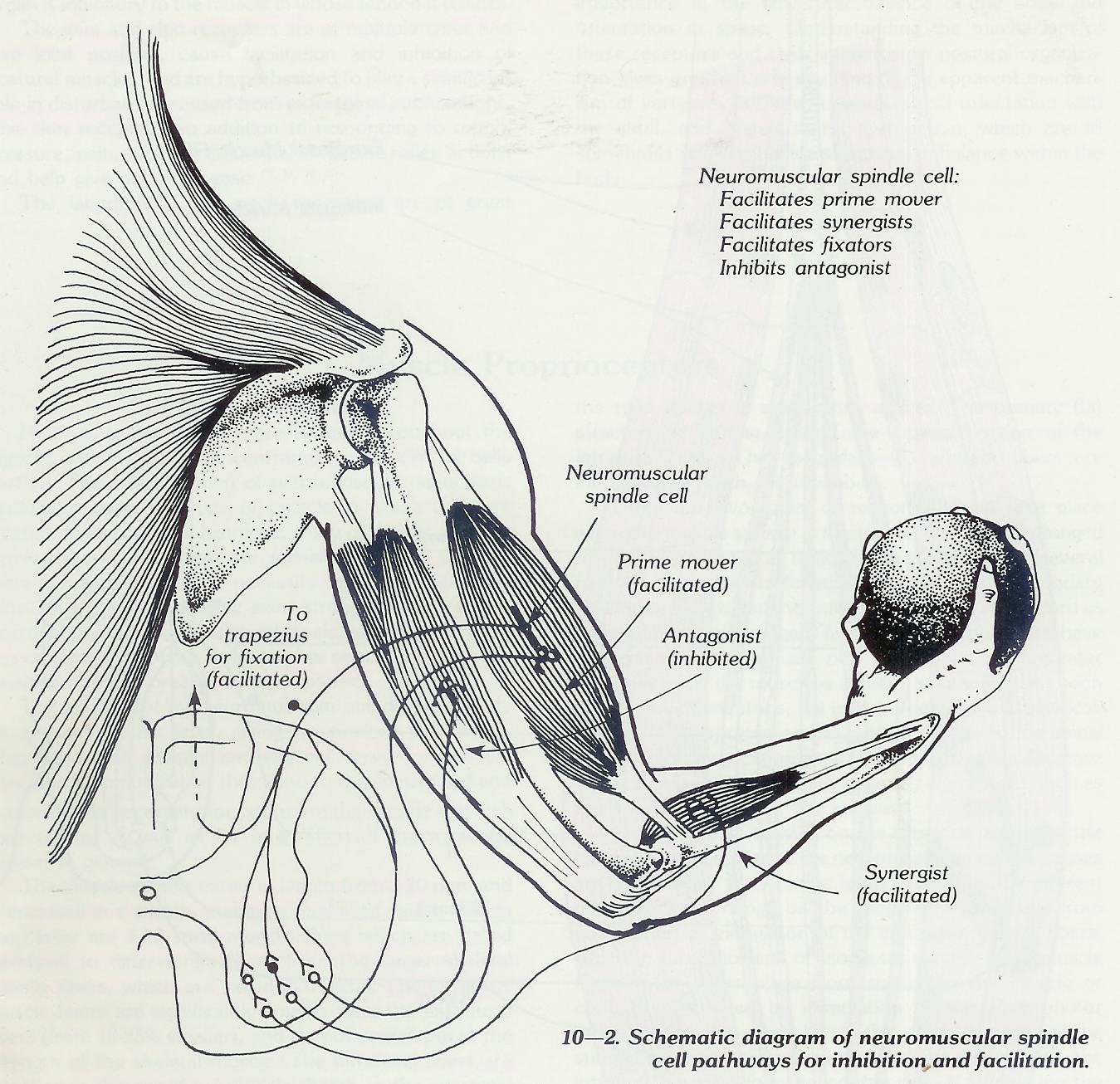{kind=link}
Muscle
structure is innervated by both sensory and motor neuron axons. Its
functions are to send proprioceptive information
about the muscle to the central nervous
system, and to respond to muscle stretching.
Anatomy Muscle spindles are found within the fleshy portions of muscles,
embedded in so-called extrafusal
muscle fibres. They are composed of 3-10 intrafusal
muscle fibres, of which there are three types:
dynamic nuclear bag fibres
(bag1 fibres) static nuclear bag fibers (bag2
fibres) nuclear chain
fibers and the axons
(are dendrites but some authors call axions because of their similarity pseudo-unipolar
type) of sensory neurons. Axons
of motor neurons
also terminate in muscle spindles; they make synapses at either or
both of the ends of the intrafusal muscle fibers
and regulate spindle sensitivity. Muscle spindles are encapsulated by
connective tissue, and are aligned parallel
to extrafusal
muscle fibers, unlike Golgi tendon
organs, which are oriented in series.
The muscle spindle has both sensory and motor components. Primary
and secondary
sensory fibers spiral around and terminate on the central portions of
intrafusal fibers, providing the sensory component of the structure via
stretch-sensitive ion-channels
of the axons. In humans, the motor component is provided by gamma motoneurons; in many other
species, beta motoneurons innervate the spindles. They cause a slight contraction
of the end portions of the intrafusal muscle fibers
when activated. The gamma (fusimotor) axons only innervate the intrafusal
muscle fibres, whereas the beta (skeletofusimotor) axons innervate both
extrafusal and ntrafusal muscle fibres. These motorneurons are classified as
static or dynamic according to their pattern of innervation and their
physiological effects. The static axons innervate the chain or bag2
fibres. The dynamic axons innervate the bag1 fibres and increase the
velocity sensitivity of the Ia afferents. [edit]
Sensitivity Modification The function of the gamma motor neuron neuromuscular
junction is not to supplement the general muscle
contraction provided by extrafusal fibers, but to modify
the sensitivity of the muscle spindle to stretch. Upon release of acetylcholine by the gamma
neuron, the end portions of the intrafusal muscle fibers
(fusiform=tapering toward each end. Spindle) contract, thus
deliberately elongating the non-contractile central portions of intrafusal muscle fibers.
This opens stretch-sensitive ion channels of the
centrally-positioned sensory axons, leading to an influx of sodium
ions. This raises the resting potential of these axons,
thereby increasing the probability of action potential firing, thus
increasing the sensitivity of the muscle spindle.[edit]
Stretch reflex When a muscle is stretched, primary sensory fibers (Group Ia
afferent neurons) of the muscle spindle respond to
both the velocity and the degree of stretch, and send this information to the spinal cord. Likewise,
secondary sensory fibers (Group II
afferent neurons) detect and send information about
the degree of stretch (but not the velocity thereof) to the CNS. This
information is transmitted monosynaptically
to an alpha efferent
motor fiber, which activates extrafusal fibers of
the muscle to contract, thereby reducing stretch, and polysynaptically
through an interneuron
to another alpha motoneuron,
which inhibits contraction in the antagonizing muscles. PNF stretching, or
proprioceptive neuromuscular facilitation, is a method of flexibility training
that reduces the automatic reflex action in order allow muscles to lengthen. [edit]
Development It is also believed that muscle spindles play a critical role in sensorimotor development.
The 3-10 intrafusal muscle fibers
(cells) are partially enclosed in connective tissue capsule which is filled
with lymph. The ends of the spindles are anchored to the endomysium and perimysium.
This means that as the extrafusal muscle fibers are stretched or contracted so are
the intrafusal muscle fibers. The spindles, intrafusal muscle fibers (cells)
are 10 to 25% smaller than the extrafusal fibers. These intrafusal fibers
measure around 2-20 mm and they are microscopic. That is they may be just under
an inch long but they are microscopically wide. As per above the end portions
of the intrafusal fibers contract (they contain actin and myosin myofilaments
which are the contractile elements of a muscle cell) while the center portion
do not contract. Although the center portion of the intrafusal fiber does not
contain contractile elements it does contain multiple cellular nuclei. The
central portion of the intrafusal fibers is called the nuclear bag because it
is bag like. There are 3-9 nuclear chain fibers and 1 to 3 nuclear bag fibers
with two types of nuclear bag fibers dynamic and static. There are 3-9 nuclear
chain fibers per muscle spindle that are half the size of the nuclear bag fibers. Their nuclei
are aligned in a chain and they excite the secondary nerve. They are static
while the nuclear bag fibers are dynamic in comparison. The name "nuclear
chain" refers to the structure of the central region of the fiber, where
the sensory axons wrap around the intrafusal fibers. As intrafusal muscle fibers, nuclear
chain fibers both send afferent innvervation and
receive efferent innervation.
The afferent innervation is via Group II and Ia neurons. These project to the nucleus proprius in the dorsal horn of the spinal cord. Efferent
innervation is via static γ neurons.
Stimulation of γ neurons causes the nuclear chain to shorten along with
the extrafusal muscle fibers.
This shortening allows the nuclear chain fiber to be sensitive to changes in
length while its corresponding muscle is flexed. As aforementioned, the
intrafusal fibers are innervated by both motor and sensory neurons.
The extrafusal skeletal muscle fibers
receive efferent (motor) neurons from the ventral horn of the gray matter in
the spinal cord or motor nuclei of the cranial nerves. These are approximate
70% of the motor fibers to the muscle and are large fibers, classified as alpha
motor neurons. The balance (30%) are gamma motor neurons which give efferent
supply to the intrafusal fibers of the neuromuscular spindle. The central
portion (called the nuclear bag) of the intrafusal fibers has either no or few
actin and myosin filaments, and consequently does not contract. It is here that
the sensory receptor area is located. It is supplied by two types of afferent
nerves-one, type 1a which is located around the nuclear bag, and usually two of
the type II fibers in the contractile part of the intrafusal fibers. The 1a
fiber is large and has a high velocity of conduction, while the type II fiber
is significantly slower. The primary (1a) attaches by curling around the
central portion of the intrafusal fiber. The secondary (II) afferent fibers are
interdigitating with the Myofibers.
There are two types of response which
take place when the muscle spindle is stretched. There is a prolonged response
referred to a tonic, which takes place for several minutes, from the stretched
stimulation of the secondary receptors. This is roughly interpreted by the
spinal cord as the magnitude of change. The primary receptors also have a
similar response but are Phasic, having a much greater response while the
muscle is actually lengthening. As soon as the movement stops, the impulse
decreases dramatically. This is interpreted as the rate of change by the spinal
cord. When the receptor area shortens, there is a decrease in the impulse
output from the primary afferent. As soon as the shortening ceases, the
impulses re-appear.
Any change of tension on the receptor
portion of the intrafusal muscle fiber of the neuromuscular spindle causes an
appraisal of the change to be sent over the afferent pathway. The change on the
receptor area can be from contraction or elongation of the extrafusal muscle
fibers, which in turn shortens or elongates the intrafusal muscle fibers. This
takes place from stretching the muscle or contraction caused by stimulation of
the alpha motor neurons. On the other hand, the receptor area can be stimulated
from gamma nerve stimulation, causing the intrafusal muscle fibers to contract,
thus stimulating the receptor area of the neuromuscular spindle cell. In
effect, the muscle spindle acts as a comparator of the lengths of the two types
of muscle fibers. There are normally sensory nerve impulses coming from the
neuromuscular spindle all the time. Changing the length of the muscle either
increases or decreases the rate of firing of the afferent nerve.
The stretch reflex is divided into two
types. The dynamic stretch reflex occurs when a quick stretching of the muscle
causes the neuromuscular spindle to be stimulated, and the monosynaptic reflex
arc causes the same muscle to contract. An example of this is the knee jerk
reflex. The static stretch reflex is from stimulation of the neuromuscular
spindle from a slow and continued stretch of the muscle, causing a less intense
reaction which causes the muscle to have an opposing contraction to the
lengthening force.
The neuromuscular spindle controls smoothness
of muscle contraction so that it does not oscillate and jerk in its motions.
This correlates with the Phasic muscles having a higher percentage of
neuromuscular spindles than the tonic weight bearing muscles of the body. The
Phasic muscles need more control because of their more intricate, dynamic
capabilities. Regulation of muscle force is also needed to hold varying weights
at specific heights. As additional weight is put on the extended arm, the
neuromuscular spindle cell monitors the increasing weight and regulates the
contracting force desired.
The neuromuscular spindle cell is
responsible for the organization of the agonist with the antagonist, synergists
and fixator muscles. There is an excitatory effect on the muscle in which the
spindle lies, facilitory effect on the synergistic and fixator muscles, and an
inhibitory effect upon the antagonist muscles.
The effect of the neuromuscular spindle
cell on the extrafusal fibers may become either hyperactive or hyperactive and
cause erroneous information to be transferred through the simple oligosynaptic
(olig=few) loops into the neuronal pools affecting this or other muscles. It is
unknown histologically what causes the neuromuscular spindle to malfunction. It
could be injury to the spindle fibers, or trauma to the capsule of the spindle
causing swelling of the spindle, with consequent mechanical pressures on the
receptor area. It could also be a lack of gliding motion of the intrafusal
fibers by an adhesion with the fibrous capsule, which is normally separated
from the intrafusal capsules by a lymph space bridged by delicate septa. The
changes in the proprioceptors could also be a trained or learned response, as
is seen in proprioceptive neuromuscular facilitation, an example of which is
the conditioning a weight lifter does for greater power.
Muscle tone
http://en.wikipedia.org/wiki/Muscle_tone
Muscle tone
(aka residual muscle tension or tonus) is the continuous and
passive partial contraction of the muscles.
It helps maintain posture
and declines during REM sleep.
Note that muscular tone is not defined as muscular shaping or the aspect
of general Human physical
appearance. Purpose Unconscious nerve impulses maintain the
muscles in a partially contracted state. If a sudden pull or stretch occurs,
the body responds by automatically increasing the muscle's tension, a reflex
which helps guard against danger as well as helping to maintain balance. The presence
of near-continuous innervation makes it clear that tonus describes a
"default" or "steady state" condition. There is, for the
most part, no actual "rest state" insofar as activation is concerned.
In terms of skeletal muscle, both the extensor muscle and flexor muscle use the term
tonus to refer to the "at rest" or normal enervation that maintains
current positions of bones.
Cardiac muscle
and smooth muscle,
although not directly connected to the skeleton also have tonus in the sense
that although their contractions are not matched with those of antagonist
muscles, their non-contractive state is characterized by (sometimes random)
enervation. [edit]
Pathological tonus Physical disorders can result in abnormally low (hypotonia) or high (hypertonia) muscle tone.
Another form of hypertonia is Paratonia, which is
associated with dementia. [edit]
Tonus in surgery In ophthalmology,
tonus may be a central consideration in eye surgery, as in the
manipulation of extraocular
muscles to repair strabismus. Tonicity
aberrations are associated with many diseases of the eye (e.g. Adie syndrome). [edit]
Tonus training Some[Cite]
present the idea that constant daily resistance training, or training at high
intensities, will increase one's muscle tone, as the neurological system
becomes more tense after constant exertion to stay in a state of greater
readiness for the tension.
Neuroscience
http://en.wikipedia.org/wiki/Portal:Neuroscience
http://en.wikipedia.org/wiki/Neuroscience
Neuroscience is a scientific discipline
that studies the structure,
function, development,
genetics, biochemistry, physiology, pharmacology, and pathology of the nervous system. Traditionally
it is seen as a branch of biological
sciences. However, recently there has been a
convergence of interest from many allied disciplines, including psychology, computer science, statistics, physics, philosophy, mathematics, and medicine. The scope of neuroscience
has now broadened to include any systematic scientific experimental and
theoretical investigation of the central and peripheral nervous system of
biological organisms. The methodologies employed by neuroscientists have been
enormously expanded, from biochemical and genetic analysis of dynamics of
individual nerve cells
and their molecular constituents to imaging representations
of perceptual and motor tasks in the brain. Furthermore, neuroscience is at the
frontier of investigation of the brain and mind. The study of the brain is
becoming the cornerstone in understanding how we perceive and interact with the
external world and, in particular, how human experience and human biology
influence each other. It is likely that the study of the brain will become one
of the central intellectual endeavors in the coming decades. The scientific study of the nervous systems underwent a
significant increase in the second half of the twentieth century, principally
due to revolutions in molecular biology, neural networks and computational
neuroscience. It has become possible to understand,
in exquisite detail, the complex processes occurring inside a single neuron
and in a network that eventually produces the intellectual behavior, cognition,
emotion and physiological responses. The task of neural science is to explain
behavior in terms of the activities of the brain. How does the brain marshal
its millions of individual nerve cells to produce behavior, and how are these
cells influenced by the environment...? The last frontier of the biological sciences--their
ultimate challenge--is to understand the biological basis of consciousness and
the mental processes by which we perceive, act, learn, and remember. — Eric Kandel, Principles
of Neural science, fourth edition
Nerve
http://en.wikipedia.org/wiki/Nerve_ending
A nerve
is an enclosed, cable-like bundle of axons (the long, slender projection of
a neuron). Neurons
are sometimes called nerve cells, though this term is technically
imprecise since many neurons do not form nerves, and nerves also include the glial cells
that ensheath the axons in myelin. Nerves are part of the peripheral
nervous system. Afferent nerves convey sensory signals to the central nervous
system, for
example from skin or organs, while efferent nerves conduct stimulatory signals from the central
nervous system to the muscles and glands. Afferent and efferent nerves
are often arranged together, forming mixed nerves. Each peripheral nerve is
covered externally by a dense sheath of connective tissue, the epineurium.
Underlying this is a layer of flat cells forming a complete sleeve, the perineurium.
Perineurial septa extend into the nerve and
subdivide it into several bundles of fibres. Surrounding each such fibre is the
endoneurial sheath. This is a tube which extends, unbroken, from the surface
of the spinal cord to the level at which the axon synapses with its muscle
fibres or ends in sensory endings. The endoneurial sheath consists of an inner
sleeve of material called the glycocalyx
and an outer, delicate, meshwork of collagen fibres. Peripheral nerves are
richly supplied with blood. Most nerves connect to the central nervous
system through
the spinal cord. The twelve cranial nerves, however, connect directly to parts of the brain. Spinal nerves are given letter-number combinations according to
the vertebra
through which they connect to the spinal column. Cranial nerves are assigned
numbers, usually expressed as Roman numerals from I to XII. In addition, most nerves and major
branches of nerves have descriptive names. Inside the central nervous system,
bundles of axons are termed tracts rather than nerves. The signals
that nerves carry, sometimes called nerve impulses, are also known as action potentials: rapidly (up to 120 m/s) traveling electrical waves,
which begin typically in the cell body of a neuron and propagate rapidly down
the axon to its tip or "terminus." The signals cross over from the
terminus to the adjacent neurotransmitter receptor through a gap called the synapse.
Motor neurons innervate or activate
muscles groups. The nerve system runs through the spinal cord. [edit] Clinical importance Damage to
nerves can be caused by physical injury, swelling (e.g. carpal tunnel
syndrome),
autoimmune diseases (e.g. Guillain-Barré
syndrome),
infection (neuritis), diabetes,
or failure of the blood vessels surrounding the nerve. Pinched nerves occur
when pressure is placed on a nerve, usually from swelling due to an injury or
pregnancy. Nerve damage or pinched nerves are usually accompanied by pain, numbness, weakness, or paralysis.
Patients may feel these symptoms in areas far from the actual site of damage, a
phenomenon called referred pain. Referred pain occurs because when a nerve is
damaged, signaling is defective from all parts of the area which the nerve
receives input, not just the site of the damage. Neurologists usually diagnose disorders of the nerves by a physical
examination,
including the testing of reflexes, walking
and other directed movements, muscle weakness, proprioception, and the sense of touch. This initial exam can be
followed with tests such as nerve conduction
study and electromyography (EMG).
Nocioceptors
http://en.wikipedia.org/wiki/Nociceptor
Detect
pain, usually as a result of physical or chemical damage to tissues. A nociceptor
is a sensory receptor that sends signals that cause
the perception of pain in response to potentially
damaging stimulus. Nociceptors are the nerve endings responsible for nociception,
one of the two types of persistent pain (the other, neuropathic pain, occurs when nerves in the central or peripheral
nervous system
are not functioning properly). When they are activated, nociceptors can trigger
a reflex.
Location Nociceptors are sensory neurons that are found in external tissues
such as skin,
cornea
and mucosa
as well as in internal organs, such as the muscle, joint, bladder
and gut.
The cell bodies of these neurons are located in either the dorsal root
ganglia or the trigeminal
ganglia. [edit] Types and functions There are
several types of nociceptors and they are classified according to the stimulus
modalities to which they respond: i.e. thermal, mechanical or chemical. Some
nociceptors respond to more than one of these modalities and are consequently
designated polymodal. Other nociceptors respond to none of these modalities
(although they may respond to stimulation under conditions of inflammation) and
have thereby earned the more poetic title of sleeping or silent nociceptors
(Kandel et al, 2000). Thermal nociceptors are activated by noxious heat or
cold, temperatures above 45°C and below 5°C (Kandel et al, 2000). Mechanical
nociceptors respond to excess pressure or mechanical deformation. Polymodal
nociceptors respond to damaging stimuli of a chemical, thermal, or mechanical
nature (Kandel et al, 2000). Nociceptors may have either Aδ fiber axons or more slowly conducting C fiber
axons. Thus, pain often comes in two phases, the first mediated by the
fast-conducting Aδ fibers and the second part due to C fibers. Silent
nociceptors do not usually fire action potentials, though they are much more likely to do so in the
presence of inflammation or damaging chemicals (Kandel et
al, 2000). Together these nociceptors allow the organism to feel pain in
response to damaging pressure, excessive heat, excessive cold and a range of
chemicals, the majority of which are damaging to the tissue surrounding the
nociceptor. [edit] Pathway Afferent
nociceptive fibers (those that send information to, rather than from
the brain) travel back to the spinal cord
where they form synapses in its dorsal horn.
The cells in the dorsal horn are divided
into physiologically distinct layers called laminae. Different fiber types form
synapses in different layers. Aδ
fibers form synapses in laminae I and V, C fibers connect with neurons in lamina
II, Aβ fibers connect with lamina IV.
Information is then sent from the spinal cord to the thalamus
and the cerebral cortex in the brain.
http://en.wikipedia.org/wiki/Ontology
In
philosophy, ontology (from the Greek ὤν, genitive ὄντος: of being (part. of εἶναι: to be) and
-λογία: science, study, theory) is the study of being
or existence and forms the basic subject matter of metaphysics. It seeks to
describe or posit the basic categories and relationships of being or existence
to define entities and types of entities within its framework. Ontology can be
said to study conceptions of reality; and, for the sake of distinction, at
least to the extent to which its counterpart, epistemology can be represented
as being a search for answers to the questions "What do you know?"
and "How do you know it?", ontology can be represented as a search
for an answer to the question "What is the nature of the knowable
things?". Some philosophers, notably of the Platonic school, contend that
all nouns refer to entities. Other philosophers contend that some nouns do not
name entities but provide a kind of shorthand way of referring to a collection
(of either objects or events). In this latter view, mind, instead of referring
to an entity, refers to a collection of mental events experienced by a person;
society refers to a collection of persons with some shared interactions, and
geometry refers to a collection of a specific kind of intellectual activity.
Any ontology must give an account of which words refer to entities, which do
not, why, and what categories result. When one applies this process to nouns
such as electrons, energy, contract, happiness, time, truth, causality, and
God, ontology becomes fundamental to many branches of philosophy.[1]
Osteoarthritis
http://en.wikipedia.org/wiki/Osteoarthritis
Osteoarthritis
/ Osteoarthrosis
(OA, also known as degenerative arthritis, degenerative joint
disease, arthrosis or in more colloquial terms "wear and
tear"), is a condition in which low-grade inflammation results in pain in
the joints, caused by wearing of the cartilage
that covers and acts as a cushion inside joints. As the bone surfaces become
less well protected by cartilage, the patient experiences pain upon weight
bearing, including walking and standing. Due to decreased movement because of
the pain, regional muscles may atrophy,
and ligaments
may become more lax. OA is the most common form of arthritis.
The word is derived from the Greek word "osteo", meaning
"of the bone", "arthro", meaning "joint",
and "itis", meaning inflammation, although many sufferers have little or no
inflammation. OA affects nearly 21 million people in the United States, accounting for 25% of visits to primary care physicians, and half of all NSAID (Non-Steroidal Anti-Inflammatory
Drugs) prescriptions. It is estimated that 80% of the
population will have radiographic evidence of OA by age 65,
although only 60% of those will be symptomatic.[1]
Treatment is with NSAIDs, local injections of glucocorticoid or hyaluronan,
and in severe cases, with joint replacement surgery. There has been no cure for OA, as
cartilage has not been induced to regenerate. However, if OA is caused by
cartilage damage (for example as a result of an injury) Autologous Chondrocyte
Implantation may be a possible treatment.[2]
Clinical trials employing tissue-engineering methods have demonstrated
regeneration of cartilage in damaged knees, including those that had progressed
to osteoarthritis.[3]
Further, in January 2007, Johns Hopkins University was offering to license a
technology of this kind, [4]
listing several clinical competitors in its market analysis.
http://en.wikipedia.org/wiki/Pacinian_corpuscle
http://en.wikipedia.org/wiki/Image:Gray935.png
{kind=link}
Pacinian
corpuscles are
one of the four major types of mechanoreceptor, responsible for sensitivity to deep pressure touch
and high frequency vibration. Location These corpuscles are found in mesenteries,
especially the pancreas, and are often found near joints. Like Ruffini endings, they are found in deep subcutaneous
tissue, and are
considered rapidly adapting receptors, which means they will not fire action
potentials throughout the duration of a stimulus but, rather, will fire briefly
at its beginning and end (Kandel et al., 2000). [edit] Structure Similar in physiology
to the Meissner's
corpuscle,
Pacinian corpuscles are larger and fewer in number than both Merkel cells and Meissner's corpuscles (Kandel et al., 2000).
The Pacinian corpuscle is ovoid shaped and approximately 1 mm in length. The
entire corpuscle is wrapped by a layer of connective tissue. It has 20 to 60 concentric lamellae composed of
fibrous connective tissue and fibroblasts, separated by gelatinous material.
The lamellae are very thin, flat, modified Schwann cells. In the center of the corpuscle is the inner bulb,
a fluid-filled cavity with a single afferent
unmyelinated nerve ending. [edit] Function Pacinian corpuscles
detect gross pressure changes and vibrations. Any deformation in the corpuscle
causes action potentials to be generated, by opening
pressure-sensitive sodium ion
channels in the axon membrane. This allows sodium
ions to influx in, creating a receptor
potential. These
corpuscles are especially susceptible to vibrations, which they can sense even
centimeters away (Kandel et al., 2000). Pacinian corpuscles cause action
potentials when the skin is rapidly indented but not when the pressure is
steady, due to the layers of connective tissue that cover the nerve ending
(Kandel et al., 2000). It is thought that they respond to high velocity changes
in joint position. Pacinian corpuscles have a large receptive field on the skin's surface with an especially sensitive
center (Kandel et al., 2000). They only sense stimuli that occur within this
field.
Paradigm
Philosophical and theoretical framework
of a scientific school or discipline within which theories, laws, and
generalizations and the experiments performed in support of them are
formulated; broadly : a philosophical or theoretical framework of any kind
Parasympathetic nervous system
http://en.wikipedia.org/wiki/Parasympathetic
The parasympathetic
nervous system (PSNS) is one of three divisions of the autonomic
nervous system (ANS).
The ANS -a subdivision of the peripheral nervous system (PNS)- is subdivided
into the sympathetic
(SNS),
parasympathetic (PSNS) and enteric (bowels)
nervous system (ENS).
Sympathetic and parasympathetic divisions
typically function in opposition to each other. But this opposition is better
termed complementary in nature rather than antagonistic. For an analogy, one
may think of the sympathetic division as the accelerator and the
parasympathetic division as the brake. The sympathetic division typically
functions in actions requiring quick responses. The parasympathetic division
functions with actions that do not require immediate reaction.
The
parasympathetic nervous system is a portion of the visceral (autonomic) branch
of the PNS (peripheral
nervous system).
The regions of the body associated with this division are the cranial and
sacral regions of the spinal cord. Specifically, cranial nerves III, VII, IX, X
(vagus n.) and in the sacral region (spinal nerves exiting from the sacrum) the
spinal nerves S2 to S4.
Similar
to the sympathetic division, the parasympathetic division also has pre- and
post- ganglionic neurons. Typically, in the parasympathetic division the ganglion
will be closer to the area of innervation - unlike the sympathetic ganglion
which form immediately lateral and inferior to the spinal nerve - making up the
so called "chain ganglion".
Photoreceptors
Detect
light on the retina of the eye
http://www.bartleby.com/107/illus848.html
Located
near the celiac plexus, below the diaphragm, stomach, liver. Located more below
the stomach on the left side of the body. See phrenic plexus
http://en.wikipedia.org/wiki/Phrenic_nerve
http://www.bartleby.com/107/210.html
http://www.bartleby.com/107/illus806.html
The
phrenic nerve arises from the third, fourth, and fifth cervical spinal nerves (C3-C5) in humans. It arises from the fifth, sixth
and seventh cervical spinal nerves (C5-7) in most domestic animals. The phrenic nerve is made up mostly of motor nerve
fibres for producing contractions of the diaphragm.
In addition, it provides sensory innervation for many components of the mediastinum
and pleura,
as well as the upper abdomen, especially the liver and gall bladder. Both
phrenic nerves run from C3, C4 and C5 along the anterior scalene muscle deep to the carotid sheath. The right phrenic nerve passes over the
right brachiocephalic
artery,
posterior to the subclavian vein, and then crosses the root of
the right lung
and then leaves the thorax by passing through the vena cava hiatus opening in the diaphragm at the level of T8. The
right phrenic nerve passes over the right atrium. The left phrenic nerve passes over the left ventricle and pierces the diaphragm separately. Both these
nerves supply motor fibres to the diaphragm and sensory fibres to the fibrous pericardium,
mediastinal
pleura and
diaphragmatic peritoneum.
The pericardiacophrenic artery and vein(s) travel with
the phrenic nerve. Pain arising from structures served by the phrenic nerve is
often "referred" to other somatic regions
served by spinal nerves C3-C5. For example, a subphrenic abscess (beneath the
diaphragm) might cause a patient to feel pain in the right shoulder. Irritation
of the phrenic nerve (or the tissues supplied by it) leads to the hiccup reflex. A hiccup is a spasmodic contraction of the
diaphram, which pulls air against the closed folds of the larynx. The phrenic nerve must be
identified during thoracic surgery and preserved. It passes
anterior to the hilum of the corresponding lung, and
therefore can be identified easily. Severing the phrenic nerve will paralyse
that half of the diaphragm. Breathing will be made more difficult but will
continue provided the other nerve is intact.
http://www.bartleby.com/107/220.html
http://www.bartleby.com/107/illus838.html
http://www.bartleby.com/107/illus848.html
http://www.bartleby.com/107/illus849.html
From
these illustrations, especially 848 it is clear that the phrenic plexus is
separate from the phrenic ganglion, as is the celiac plexus from the celiac
ganglion although some of these structures are not well defined. See phrenic ganglion More
centrally located below the liver near the celiac plexus. The phrenic plexus
(plexus phrenicus) accompanies the inferior phrenic artery to the diaphragm,
some filaments passing to the suprarenal gland. It arises from the upper part
of the celiac ganglion, and is larger on the right than on the left side. It
receives one or two branches from the phrenic nerve. At the point of junction
of the right phrenic plexus with the phrenic nerve is a small ganglion
(ganglion phrenicum). This plexus distributes branches to the inferior vena
cava, and to the suprarenal and hepatic plexuses.
Pleural cavity (See Pulmonary pleura Pleura)
http://en.wikipedia.org/wiki/Pleur%C3%A6
http://en.wikipedia.org/wiki/Image:Gray965.png
{kind=link}
The lungs are surrounded by two membranes,
the pleurae. The outer pleura is attached to the chest wall
and is known as the parietal pleura; the inner one is attached to the
lung and other visceral tissues and is known as the visceral
pleura. In between the two is an actual thin space known as the pleural
cavity or pleural space. It is filled with pleural fluid, a serous fluid produced by the pleura. A normal 70 kg human has
approximately 12-15 mL of pleural fluid. Pleural fluid serves several
functions. It lubricates the pleural surfaces and allows the pleural layers to
slide against each other easily during respiration. Pleural fluid also provides
the surface tension that keeps the lung surface in close apposition with the
chest wall. This allows optimal inflation of alveoli
during respiration. It also directly transmits pressures from the chest wall to
the visceral pleural surface (and hence, the lung). Therefore, movements of the
chest wall during breathing are coupled closely to movements of the lungs. The
parietal pleura is highly sensitive to pain; the visceral pleura is not. The
visceral pleura has a dual blood supply from the bronchial
and pulmonary arteries. In normal pleurae, most fluid
is produced by the parietal circulation (intercostal
arteries) via bulk flow
and reabsorbed by the lymphatic system. Thus, pleural fluid is continuously produced and
reabsorbed. The rate of reabsorption may increase up to 40x before significant
amounts of fluid accumulate within the pleural space. In humans, there is no
anatomical connection between the left and right pleural cavities, so in cases
of pneumothorax (see below), the other hemithorax will still be able to
function normally.
Pulmonary pleura (See Pleural
cavity Pleura)
http://en.wikipedia.org/wiki/Pulmonary_pleura
http://en.wikipedia.org/wiki/Image:Gray968.png
Each
lung is invested by an exceedingly delicate serous membrane, the pleura, which is arranged in the form of a
closed invaginated
sac. A portion of the serous
membrane covers
the surface of the lung and dips into the fissures between its lobes; it is
called the pulmonary pleura (or visceral pleura). The visceral pleura is
attached directly to the lungs. Visceral pleura is the innermost of the two
layer of pleural membranes investing the lungs. It consists of a smooth layer
of continuous mesothelial cells. It is deep to the
parietal pleura (fibrous connective tissue); a thin layer of serous fluid
intervenes between the two in the potential space of the pleural cavity. The
visceral and parietal pleura only merge together as a layer at root of the
lung. Elsewhere, the fluid lubricant within the pleural cavity permits both
layers to slide freely over each other. The visceral pleura closely follows the
underlying lung surface. It passes down into fissures between lobes; along
these fissures, visceral pleura is apposed to visceral pleura.
http://en.wikipedia.org/wiki/Pericardium
http://en.wikipedia.org/wiki/Image:Gray489.png
{kind=link}
http://en.wikipedia.org/wiki/Image:Gray968.png
The pericardium is a
double-walled sac that contains the heart
and the roots of the great vessels.
There are two layers to this sac: the fibrous pericardium and the serous
pericardium. The serous pericardium, in turn, is divided into two layers; in
between these two layers there is a potential space called the pericardial cavity.
The fibrous pericardium is the most superficial layer. It is a dense connective tissue, protecting the
heart, anchoring it to the surrounding walls, and preventing it from
overfilling with blood.
It is continuous with the outer
adventitial layer (adventitial)
of the neighboring great blood vessels. The serous
pericardium is deeper than the fibrous pericardium. It contains two layers,
both of which function in lubricating the heart to prevent friction from
occurring during heart activity. The layer next to the fibrous pericardium is
the parietal layer. The
layer deep to the fibrous pericardium is the visceral
layer. When this layer comes into contact with the heart (not the great
vessels), it is known as the epicardium. Together these
two layers form a continuous uninterrupted membrane. Between these two layers
exists a small cavity called the pericardial cavity, which contains a supply of
serous fluid.The serous
fluid that is found in this space is known as the pericardial fluid.
http://en.wikipedia.org/wiki/Peritoneum
In higher vertebrates, the peritoneum
is the serous membrane
that forms the lining of the abdominal cavity - it covers
most of the intra-abdominal organs. It is composed of a layer of mesothelium supported by a
thin layer of connective tissue.
The peritoneum both supports the abdominal organs and serves as a conduit for
their blood and lymph
vessels and nerves. Although they
ultimately form one continuous sheet, two types or layers of peritoneum and a
potential space between them are referenced: The outer layer, called the parietal
peritoneum, is attached to the abdominal wall. The inner
layer, the visceral peritoneum, is wrapped around the internal organs that are
located inside the abdominal cavity. The potential space between these two
layers is the peritoneal cavity; it is filled with a small amount (about
50 ml) of slippery serous fluid that allows the
two layers to slide freely over each other. The term mesentery is often used
to refer to a double layer of visceral peritoneum. There are often blood
vessels, nerves, and other structures between these layers. It should be noted
that the space between these two layers is technically outside of the
peritoneal sac, and thus not in the peritoneal cavity. There are two main
regions of the peritoneum, connected by the epiploic foramen: the greater sac (or general
cavity of the abdomen), represented in red in the diagrams above. the lesser sac (or omental
bursa), represented in blue. The lesser sac is divided into two
"omenta": The lesser omentum (or gastrohepatic)
is attached to the lesser curvature of the stomach and the liver.
The greater omentum
(or gastrocolic) hangs from the greater curve of the stomach and loops
down in front of the intestines
before curving back upwards to attach to the transverse colon. In effect it
is draped in front of the intestines like an apron and may serve as an
insulating or protective layer. The mesentery is the part of
the peritoneum through which most abdominal organs are attached to the abdominal wall and supplied
with blood and lymph
vessels and nerves.
Phrenic plexus
http://en.wikipedia.org/wiki/Phrenic_plexus
The phrenic
plexus accompanies the inferior phrenic
artery to the diaphragm,
some filaments passing to the suprarenal gland. It arises from the upper part of the celiac ganglion, and is larger on the right than on the left side.
It receives one or two branches from the phrenic nerve. At the point of junction of the right phrenic
plexus with the phrenic nerve is a small ganglion (ganglion phrenicum).
This plexus distributes branches to the inferior vena cava, and to the suprarenal
and hepatic plexuses.
http://en.wikipedia.org/wiki/Physics
Physics
(Greek: φύσις (phúsis), "nature" and
φυσικῆ (phusiké), "knowledge of
nature") is the branch of science concerned with discovering and
characterizing universal laws that govern matter, energy, space, and time.
Discoveries in physics resonate throughout the natural sciences, and physics
has been described as the "fundamental science" because other fields
such as chemistry and biology investigate systems whose properties depend on
the laws of physics.[1] The emergence of physics as a science distinct from
natural philosophy began with the scientific revolution of the 16th and 17th
centuries, and continued through the dawn of modern physics in the early 20th
century. The field has continued to expand, with a growing body of research
leading to discoveries such as the Standard Model of fundamental particles and
a detailed history of the universe, along with revolutionary new technologies
like nuclear energy and semiconductors. Research today progresses on a vast
array of topics, including high-temperature superconductivity, quantum
computing, the search for the Higgs boson, and the attempt to develop a theory
of quantum gravity. Grounded in observations and experiments and supported by
deep, far-reaching theories, physics has made a multitude of contributions to
science, technology, and philosophy.
Placebo
http://en.wikipedia.org/wiki/Placebo
A placebo is a preparation which is pharmacologically inert but which may have a medical effect based solely on the power of suggestion, a response known as the placebo effect or placebo response. It may be administered through ingestion, injection, inhalation, insertion into a body cavity, or applied topically.[1] The term placebo effect (as distinct from the more correct term placebo response) was introduced by T. C. Graves in 1920 "because it is the subject that has the subject-centred response. It is not the administered substance that generates the observed effect." Sometimes known as non-specific effects or subject-expectancy effects, a so-called placebo effect occurs when a patient's symptoms are altered in some way (i.e., alleviated or exacerbated) by an otherwise inert treatment, due to the individual expecting or believing that it will work. Some people consider this to be a remarkable aspect of human physiology; others consider it to be an illusion arising from the way medical experiments are conducted.
Placebo Analgesia
Careful studies have shown that the placebo effect can alleviate pain,
although the effect is more pronounced with pre-existing pain than with
experimentally induced pain. People can be conditioned to expect analgesia in
certain situations. When those conditions are provided to the patient, the
brain responds by generating a pattern of neural activity that produces
objectively quantifiable analgesia. (Benedetti 2003, Wager 2004) Evans argued
that the placebo effect works through a suppression of the acute phase
response, and as a result does not work in medical conditions that do not
feature this. (Evans 2005) The acute phase response consists of inflammation
and sickness behaviour: Four classic signs of ‘inflammation’: tumor, rubor,
calor, and dolor – (Latin for "swelling, redness, heat, and pain").
Sickness behaviour: lethargy, apathy, loss of appetite, and increased
sensitivity to pain.
http://en.wikipedia.org/wiki/Pleura
The
lungs
are surrounded by two membranes,
the pleurae. The outer pleura is attached to the chest
wall and is known as the parietal pleura;
the inner one is attached to the lung and other visceral
tissues and is known as the visceral pleura. In between the two is an
actual thin space known as the pleural cavity or pleural space.
It is filled with pleural fluid, a serous
fluid (serous
membrane) produced by the pleura. A normal 70 kg
human has approximately 12-15 mL of pleural fluid. Pleural fluid serves several
functions. It lubricates the pleural surfaces and allows the pleural layers to
slide against each other easily during respiration. Pleural fluid also provides
the surface tension that keeps the lung surface in close apposition with the
chest wall. This allows optimal inflation of alveoli
during respiration. It also directly transmits pressures from the chest wall to
the visceral pleural surface (and hence, the lung). Therefore, movements of the
chest wall during breathing are coupled closely to movements of the lungs. The
parietal pleura is highly sensitive to pain; the visceral pleura is not. The
visceral pleura has a dual blood supply from the bronchial
and pulmonary arteries.
In normal pleurae, most fluid is produced by the parietal circulation (intercostal arteries)
via bulk
flow and reabsorbed by the lymphatic
system. Thus, pleural fluid is continuously
produced and reabsorbed. The rate of reabsorption may increase up to 40x before
significant amounts of fluid accumulate within the pleural space. In humans,
there is no anatomical connection between the left and right pleural cavities,
so in cases of pneumothorax (see below), the other hemithorax will still be
able to function normally.
http://en.wikipedia.org/wiki/Plexus
In many animals the
processes of neurons join together to form a
plexus or nerve net. This is the characteristic form of nervous system in the coelenterates and persists with
modifications in the flatworms. The nerves of the radially symmetric echinoderms also take this form, where
a plexus underlies the ectoderm of these animals and deeper
in the body other nerve cells form plexuses of
limited extent.
In vertebrates nerves branch and rejoin in
some parts of the body, for example the brachial plexus made up of the spinal nerves which enter the arm
and the solar
plexus
above the stomach.
Almost a hundred
such plexuses have been named in the human body, but the four primary nerve plexuses are the cervical plexus, brachial plexus, lumbar plexus, and the sacral plexus.
Posterior horn
http://en.wikipedia.org/wiki/Dorsal_horn
http://en.wikipedia.org/wiki/Image:Medulla_spinalis_-_Section_-_English.svg
{kind=link}
The posterior
horn (posterior column, posterior cornu, dorsal horn, spinal
dorsal horn) of the spinal cord is the dorsal (more towards
the back) grey matter of the spinal cord. It receives several types of sensory
information from the body, including light
touch, proprioception, and vibration. This information is sent
from receptors of the skin, bones, and joints through sensory neurons whose cell bodies lie in the dorsal root ganglion.
Pseudoscience [35]
http://en.wikipedia.org/wiki/Pseudoscience
http://www.skeptic.com/reading_room/debates/afterlife.html
Pseudoscience
is any body of knowledge, methodology, belief, or practice that claims to be
scientific or is made to appear scientific, but does not adhere to the basic
requirements of the scientific method. The term pseudoscience is based on the
Greek root pseudo- (false or pretending) and science (derived from Latin
scientia, meaning knowledge). The first recorded use was in 1843 by French
physiologist François Magendie considered a pioneer in experimental physiology.
The term has negative connotations, because it is used to indicate that
subjects so labeled are inaccurately or deceptively portrayed as science.
Accordingly, those labeled as practicing or advocating a
"pseudoscience" normally reject this classification. As it is taught
in certain introductory science classes, pseudoscience is any subject that
appears superficially to be scientific or whose proponents state is scientific
but nevertheless contravenes the testability requirement, or substantially
deviates from other fundamental aspects of the scientific method. Professor Paul DeHart Hurd argued that a large part of gaining
scientific literacy is being able to distinguish science from pseudo-science
such as astrology, eugenics, quackery, the occult, and superstition.[9] Certain
introductory survey classes in science take careful pains to delineate the
objections scientists and skeptics have to practices that make direct claims
contradicted by the scientific discipline in question. Beyond the initial
introductory analyses offered in science classes, there is some epistemological
disagreement about whether it is possible to distinguish "science"
from "pseudoscience" in a reliable and objective way. Pseudoscience’s
may be characterized by the use of vague, exaggerated or untestable claims, over-reliance
on confirmation rather than refutation, lack of openness to testing by other
experts, and a lack of progress in theory development.
Using
the accurate findings of scientific inquiry to draw unsupported false
conclusions and or conversely claims or appears to be scientific without
adhering to the scientific method.
Proprioceptors
http://en.wikipedia.org/wiki/Proprioceptors
Provide
information about body position and movement. Such sensations give us
information about muscle tension, the position and activity of our joints, and
equilibrium. These receptors are located in muscles, tendons, joints, and the
internal ear.
Proprioception (PRO-pree-o-SEP-shun
(IPA
pronunciation: [ˈpɹopɹiːoˌsɛpʃən]);
from Latin proprius,
meaning "one's own" and perception) is the sense of the
relative position of neighbouring parts of the body. Unlike the six exteroceptive senses
(sight, taste, smell, touch, hearing, and balance) by
which we perceive the outside world, and interoceptive
senses, by which we perceive the pain and the stretching of internal organs,
proprioception is a third distinct sensory modality that provides feedback
solely on the status of the body internally. It is the sense that indicates
whether the body is moving with required effort, as well as where the various
parts of the body are located in relation to each other. The Position-Movement
sensation was originally described in 1557 by Julius Caesar Scaliger as a
'sense of locomotion'. Much later in 1826 Charles
Bell
expounded the idea of a 'muscle sense' and this is credited with being one of
the first physiologic feedback mechanisms. Bell's idea was that commands were
being carried from the brain to the muscles, and that reports on the muscle's
condition would be sent in the reverse direction. Later, in 1880, Henry Charlton Bastian suggested
'kinaesthesia' instead of 'muscle sense' on the basis that some of the afferent
information (back to the brain) was coming from other structures including
tendon, joints, skin, and muscle. In 1889, Alfred Goldscheider
suggested a classification of kinaesthesia into 3 types: muscle, tendon, and
articular sensitivity. In 1906, Sherrington published a landmark work which
introduced the terms 'proprioception' 'interoception', and 'exteroception'. The
'exteroceptors' being the organs responsible for information from outside the
body such as the eyes, ears, mouth, and skin. The interoceptors then gave
information about the internal organs, while 'proprioception' was awareness of
movement derived from muscular, tendon, and articular sources. Such a system of
classification has kept physiologists and anatomists searching for specialised
nerve endings which transmit data on joint capsule and muscle tension (such as
muscle spindles and Pacini corpuscles).
Receptor
Potential
A
phenomenon that has many characteristics similar to a generator potential is
called a receptor potential. When a receptor cell connected to a neuron via a
synapse is adequately stimulated, the receptor responds by depolarization of
its membrane. This depolarization is called a receptor potential. Once
developed, a receptor potential stimulates the release of neurotransmitters
from a receptor cell, which alters the permeability of the neuron’s membrane. If
the neuron becomes depolarized to threshold, a nerve action potential is
triggered.
Rene Descartes
(1596-1650)
http://en.wikipedia.org/wiki/Ren%C3%A9_Descartes
French
Mathematician and philosopher-established the necessity for a rigorous,
rational analysis and explanation of natural phenomena)(used inference (the act
of passing from one proposition, statement, or judgment considered as true to
another whose truth is believed to follow from that of the former)) [36] [37] [38]
“I think, therefore I am””there is nothing which gives me assurance of their
truth beyond this; that I see very clearly that in order to think it is
necessary to exist.”
René
Descartes (French IPA: [ʁə'ne
de'kaʁt]) (March 31, 1596 – February
11, 1650), also known as Renatus Cartesius (latinized form), was a highly
influential French philosopher, mathematician, scientist, and writer. Dubbed
the "Father of Modern Philosophy," and the "Father of Modern
Mathematics," much of subsequent western philosophy is a reaction to his
writings, which have been closely studied from his time down to the present
day. His influence in mathematics is also apparent, the Cartesian coordinate
system that is used in plane geometry and algebra being named for him, and he
was one of the key figures in the Scientific Revolution.
http://en.wikipedia.org/wiki/Right_atrium
The
right atrium (in older texts termed the "right auricle") is
one of four chambers (two atria and two ventricles) in
the human heart. It
receives de-oxygenated blood from
the superior and inferior vena
cavae
and the coronary sinus, and
pumps it into the right ventricle
through the tricuspid valve. The sinoatrial
node
(SAN) is located within this chamber next to the vena cava. This is a group of
pacemaker cells which spontaneously depolarise to create an Action Potential.
The cardiac action potential then spreads across both atria causing them to
contract forcing the blood they hold into their corresponding ventricles. In
early life, when a fetus is in the womb, the right atrium
has a hole within its septum through to the left atrium, this makes them
continuous with each other which is essential for foetal circulation. This
junction is called the “Foramen Ovale”. Once born (usually within a year's
time) the Foreman Ovale seals over and it is renamed as the “Fossa Ovalis”. The
Fossa Ovalis is seen as an embryonic remnant. The right atrium also holds the
coronary sinus which is the opening of the vein that drains the myocardium
itself. Attached to the right atrium is the right auricular appendix.
Righting Reflexes
righting
reflexes [39]
[40] [41] [42] [43] [44] [45] [46] [47]
The
ability to assume an optimal position when there has been a departure from it)
(facilitated by equilibrium Proprioceptors).
SCIENCE
Got an
idea for how nature works and want to find out if it is real and true. Use
scientific method to find out-formulate testable hypotheses, test these
hypotheses under controlled conditions, Put together those hypotheses that are
correct to formulate theories. Inductive reasoning formulates these hypothesis
only after empirical observation and deductive reasoning begins with testable hypothesis
and looks to experiment for conformation. Alexander follows an incomplete path
(unscientific) he formulates theories (Paradigm) based on anecdotal experience
(uncontrolled-no objective empirical observation) and or makes subjective
(uncontrolled-non objective) observations to theories. This process runs the
risk that imagination exceeds reality and you will see what you want to see. It
may be a successful strategy since suggestion can produce healing and the
marketplace may reward the visionary even if they are wrong about the details.
When the vision is appealing to consumer it is rewarded financially. (?)
http://en.wikipedia.org/wiki/Scientific_method
Scientific
method is a body
of techniques for investigating phenomena, acquiring new knowledge, or correcting and integrating
previous knowledge. It is based on gathering observable, empirical and measurable evidence subject to specific principles
of reasoning,[1] the collection of data through observation and experimentation, and the formulation and testing
of hypotheses.[2]
Although
procedures vary from one field
of inquiry to
another, identifiable features distinguish scientific inquiry from other
methodologies of knowledge. Scientific researchers propose hypotheses as explanations of phenomena,
and design experimental studies to test these hypotheses. These
steps must be repeatable in order to predict dependably any future results. Theories that encompass wider domains of
inquiry may bind many hypotheses together in a coherent structure. This in turn
may help form new hypotheses or place groups of hypotheses into context.
Among
other facets shared by the various fields of inquiry is the conviction that the
process must be objective to reduce a biased interpretation of the results.
Another basic expectation is to document, archive and share all data and methodology so it
is available for careful scrutiny by other scientists, thereby allowing other
researchers the opportunity to verify results by attempting to reproduce them. This practice, called full
disclosure, also allows statistical measures of the reliability of these data to be established.
http://en.wikipedia.org/wiki/Serous_membrane
In
anatomy, a serous membrane, or serosa,
is a smooth membrane (Example= Pulmonary pleura) consisting of a thin layer of cells which excrete a fluid, known as serous
fluid. Serous
membranes line and enclose several body cavities, known as serous cavities,
where they secrete a lubricating fluid which reduces friction from muscle movement.
Serosa is not to be confused with adventitia, a connective tissue layer which
binds together structures rather than reducing friction between them. Each
serous membrane is composed of a secretory epithelial layer and a connective
tissue layer
underneath. The epithelial layer, known as mesothelium, consists of a single layer of avascular flat nucleated cells (simple squamous
epithelium)
which produce the lubricating serous fluid. This fluid has a consistency
similar to thin mucous.
These cells are bound tightly to the underlying connective tissue. The connective
tissue layer provides the blood
vessels and nerves for the overlying secretory
cells, and also serves as the binding layer which allows the whole serous
membrane to adhere to organs and other structures.
http://en.wikipedia.org/wiki/Sigmund_Freud
Sigmund
Freud (IPA: [ˈziːkmʊnt
ˈfʁɔʏt]), born Sigismund Schlomo Freud
(May 6, 1856 – September 23, 1939), was an Austrian neurologist and
psychiatrist who co-founded the psychoanalytic school of psychology. Freud is
best known for his theories of the unconscious mind, especially involving the
mechanism of repression; his redefinition of sexual desire as mobile and
directed towards a wide variety of objects; and his therapeutic techniques,
especially his understanding of transference in the therapeutic relationship
and the presumed value of dreams as sources of insight into unconscious
desires.[citation needed] He is commonly referred to as "the father of
psychoanalysis" and his work has been highly influential — popularizing
such notions as the unconscious, defense mechanisms, Freudian slips and dream symbolism
— while also making a long-lasting impact on fields as diverse as literature,
film, Marxist and feminist theories, philosophy, and psychology. However, his
theories remain controversial and disputed by numerous critics.
Smooth muscle
http://en.wikipedia.org/wiki/Smooth_muscle
Muscle tissue that lacks cross
striations, is made up of elongated spindle-shaped cells having a central
nucleus, and is found especially in vertebrate hollow organs and structures (as
the digestive tract and bladder) as thin sheets performing functions not
subject to direct voluntary control and in all or most of the musculature of
invertebrates other than arthropods. Smooth muscle is a type of non-striated
muscle, found within the "walls" of hollow organs and elsewhere like
the bladder and abdominal cavity, the uterus, male and female reproductive
tracts, the gastrointestinal tract, the respiratory tract, the vasculature, the
skin and the ciliary muscle and iris of the eye. The glomeruli of the kidneys
contain a smooth muscle like cell called the mesangial cell. Smooth muscle is
fundamentally different from skeletal muscle and cardiac muscle in terms of
structure and function.
Smooth muscle
is a type of non-striated
muscle, found within
the "walls" of hollow organs and elsewhere
like the bladder
and abdominal cavity, the uterus,
male and female reproductive tracts, the gastrointestinal
tract, the respiratory tract, the
vasculature, the skin and the ciliary muscle and iris of the eye. The glomeruli of the kidneys
contain a smooth muscle like cell called the mesangial cell. Smooth muscle
is fundamentally different from skeletal muscle and cardiac muscle in terms of
structure and function. Structure
Smooth muscle fibers are spindle shaped,
and like all muscle, can contract and relax. In the relaxed state, each cell is
spindle-shaped, 20-500 micrometers long and 5 micrometers wide.[1] There are two
types of smooth muscle arrangements in the body: multi-unit and single-unit.
The single-unit type, also called unitary smooth muscle, is far more
common. Whereas the former presents itself as distinct muscle fibers that are
usually innervated by their own nerve fibers, the latter operate as a single
unit and are arranged in sheets or bundles. Unitary smooth muscle is also
commonly referred to as visceral
smooth muscle because it it found in the walls
of the viscera, or internal organs, of the body, including the intestines, ducts such as
the bile ducts, ureters
and oviducts, and most blood vessels.[2] Unitary smooth
muscle can be further divided into phasic and tonic. The cells that compose
smooth muscle generally have single nuclei. The cells are
generally arranged in sheets or bundles and connected by gap junctions. In order to
contract the cells contain intracellular contractile filamentous proteins
called actin and myosin.
While the filaments are essentially the same in smooth muscle as they are in
skeletal and cardiac muscle, the way they are arranged is different (and some
regulatory proteins are different). The smooth muscle cell contains less
protein than a typical striated muscle cell and much less myosin. The actin
content is similar so the ratio of actin to myosin is ~6:1 in striated muscle
and ~15:1 in smooth muscle. Smooth muscle does not contain the proteins
troponin or titin, and caldesmon and calponin are significant proteins
expressed witin smooth muscle. As non-striated muscle, the actin and myosin is
not arranged into distinct sarcomeres that form
orderly bands throughout the muscle cell. However there is an organized
cytoskeleton consisting of the intermediate filament proteins vimentin and
desmin, myosin filaments and actin thin filaments. Actin filaments attach to
the sarcolemma by focal adhesions or attachment plaques and attach to other actin
filaments via dense bodies (acting much like Z-lines in striated muscle).
Evidence indicates that smooth muscle myosin filaments are not bipolar with a
central bare zone as in striated muscle, but is either side-polar or row-polar
and have no bare zone. Some smooth muscle preparations can be visualized
contracting in a spiral corkscrew fashion, and contractile proteins can
organize into zones of actin and myosin along the axis of the cell. The
sarcolemma possess microdomains specialized to cell signalling events and ion
channels called caveolae. These invaginations in the sarcoplasma contain a host
of receptors
(prostacyclin, endothelin, serotonin, muscarinic
receptors, adrenergic receptors), second messenger generators
(adenylate cyclase, Phospholipase C), G proteins (RhoA, G alpha), kinases (rho
kinase-ROCK, Protein kinase C, Protein Kinase A), ion channels (L type Calcium
channels, ATP sensitive Potassium channels, Calcium sensitive Potassium
channels) in close proximity. The caveolae are often in close proximity to
sarcoplasmic reticulum or mitochondria and have been proposed to organize
signaling molecules in the membrane. [edit]
Function Muscle follows its function: to maintain organ dimensions against and
cells are fastened to one another via adherens
junctions. Consequently, cells are mechanically
coupled to one another such that contraction of one cell invokes some degree of
contraction in an adjoining cell. Gap junctions couple adjacent cells
chemically, facilitating the spread of chemicals (e.g., calcium) in single-unit smooth muscle.
Smooth muscle-containing tissue often
must be stretched, so elasticity is an important attribute of smooth muscle.
Smooth muscle cells may secrete a complex extracellular matrix containing collagen (predominantly
types I and III), elastin,
glycoproteins,
and proteoglycans.
These fibers with their extracellular matrices contribute to the viscoelasticity of these
tissues. Smooth muscle may contract spontaneously or be induced by a number of
physiochemical agents (e.g., hormones, drugs, neurotransmitters). Smooth
muscles have been divided into "multi-unit" and "visceral"
types or into "phasic" and "tonic" types based on the
characteristics of the contractile patterns. It may contract phasically
with rapid contraction and relaxation, or tonically
with slow and sustained contraction. The reproductive, digestive, respiratory,
and urinary tracts, skin, eye, and vasculature all contain this muscle type.
For example, contractile function of vascular smooth muscle is critical to
regulating the lumenal diameter of the small arteries-arterioles called
resistance vessels. The resistance arteries contribute significantly to setting
the level of blood pressure. Smooth muscle contracts slowly and may maintain
the contraction (tonically) for prolonged periods in blood vessels,
bronchioles, and some sphincters. In the digestive tract, smooth muscle
contracts in a rhythmic peristaltic fashion. It
rhythmically massages products through the digestive tract as the result of
phasic contraction. [edit]
Contraction and Relaxation Basics Smooth muscle contraction is caused by the
sliding of myosin and actin filaments (a sliding filament mechanism) over each
other. The energy for this to happen is provided by the hydrolysis of ATP.
Myosin functions as an ATPase utilizing ATP to produce a molecular
conformational change of part of the myosin and produces movement. Movement of
the filaments over each other happens when the globular heads protruding from
myosin filaments attach and interact with actin filaments to form crossbridges.
The myosin heads tilt and drag along the actin filament a small distance (10-12
nm). The heads then release the actin filament and adopt their original
conformation. They can then re-bind to another part of the actin molecule and
drag it along further. This process is called crossbridge cycling and is the
same for all muscles (see muscle
contraction). Unlike cardiac and skeletal muscle,
smooth muscle does not contain the calcium binding protein troponin.
Contraction is initiated by a calcium regulated phosphorylation of myosin,
rather than a calcium activated troponin system. Crossbridge cycling cannot
occur until the myosin heads have been activated to allow crossbridges to form.
The myosin heads are made up of heavy chains and light protein chains. When the
light chains are phosphorylated it becomes active and will allow contraction to
occur. The enzyme that phosphorylates the light chains is called myosin light
chain kinase (MLCK). In order to control
contraction, MLCK will only work when the muscle is stimulated to contract.
Stimulation will increase the intracellular concentration of calcium ions.
These bind to a molecule called calmodulin and form a
calcium-calmodulin complex. It is the complex that will bind to MLCK to
activate it, allowing the chain of reactions for contraction to occur. The
phosphorylation of the light chains by MLCK is countered by a myosin light
chain phosphatase which dephosphorylates the myosin light chains and inhibits
the contraction. In general, the relaxation of smooth muscle is by cell
signalling pathways that increase the myosin phosphatase activity, decrease the
intracellular calcium levels, and/or hyperpolarize the smooth muscle. [edit] Contraction and
Relaxation Advanced Muscle can be characterized as two types: tonic and phasic
which describes their response to depolarizing high potassium solutions. Tonic
smooth muscle contracts and relaxes slowly and exhibits force maintenance such
as vascular smooth muscle. Force maintenance is the maintaining of a
contraction for a prolonged time with little energy utilization. The phasic
smooth muscle contracts and relaxes rapidly such as gut smooth muscle. This phasic response
is useful to massage substances through the lumen of the gastrointestinal tract
during peristalsis. Vascular smooth muscle (walls of arteries and veins) and
visceral smooth muscle (wall of gastrointestinal tract, urogenital tract, iris)
is another distinction in common use to discriminate the kind of smooth muscle.
Contractions in vertebrate smooth muscle can be initiated by stretch, gap
junction electrical, and neural and humoral receptor mediated agents (acetylcholine, endothelin, etc.). Smooth
muscle in the gastrointestinal and urogenital tracts is regulated by the
enteric nervous system and by peristaltic pacemaker cells -- the interstitial
cells of Cajal. Stretch, neural and humoral
agents, and gap junction activity that depolarize the sarcolemma increase
intracellular calcium. Extracellular calcium enters through L
type calcium channels and intracellular
calcium is released from stored calcium in the sarcoplasmic
reticulum. Calcium release from the sarcoplasmic
reticulum is through Ryanodine
receptor channels (calcium sparks) by a redox
process and inositol
triphosphate receptor channels by the second messenger
inositol triphosphate. The intracellular calcium binds with calmodulin which then
binds and activates myosin-light
chain kinase. The calcium-calmodulin-myosin
light chain kinase complex phosphorylates
the 20 kilodalton
(kd) myosin light chains on amino acid residue-serine 19 to initiate
contraction. The phosphorylation of the myosin light chains then allows the
myosin ATPase to function. The thin filament associated proteins caldesmon and
calponin are also believed to serve a function in contractility within smooth
muscle. Phosphorylation of the 20 kd myosin
light chains correlates well with the shortening
velocity of smooth muscle. During this period there is a rapid burst of energy
utilization as measured by oxygen consumption. Within a few minutes of
initiation the calcium level markedly decrease, 20 kd myosin light chains
phosphorylation decreases, and energy utilization decreases and the muscle can relax,
however there is a sustained maintenance of force in vascular smooth muscle.
The sustained phase has been attributed to slowly cycling dephosphorylated
myosin crossbridges and has been termed latch-bridges. During contraction of
muscle, rapidly cycling crossbridges form between activated actin and
phosphorylated myosin generating force. During the sustained phase,
phosphorylation levels decline and slow cycling dephosphorylated crossbridges
act as latch bridges to contribute to maintaining the force at low energy
costs. Other cell signalling pathways and protein kinases (Protein kinase C,
ROCK kinase, Zip kinase, Focal adhesion kinases) have been implcated and actin
polymerization dynamics plays a role in force maintenance. While myosin light
chain phosphorylation correlates well with shortening velocity, other cell
signalling pathways have been implicated in the development of force and
maintenance of force. Notably the phosphorylation of specific tyrosine residues
on the focal adhesion adapter protein-paxillin by specific tyrosine kinases has
been demonstrated to be essential to force development and maintenance.
Phosphorylation of the 20kd myosin light chains is counteracted by a myosin
light chain phosphatase that dephosphorylates the myosin light chains. Isolated
preparations of vascular and visceral smooth muscle contract with depolarizing
high potassium balanced saline generating a certain amount of contractile
force. The same preparation stimulated in normal balanced saline with an
agonist such as endothelin or serotonin will generate more contractile force.
This increase in force is termed calcium sensitization. The myosin light chain
phosphatase is inhibited to increase the gain or sensitivity of myosin light
chain kinase to calcium. There are number of cell signalling pathways believed
to regulate this decrease in myosin light chain phosphatase: a RhoA-Rock kinase
pathway, a Protein kinase C-Protein kinase C potentiation inhibitor protein 17
(CPI-17) pathway, telokin, and a Zip kinase pathway. Further Rock kinase and
Zip kinase have been implicated to directly phosphorylate the 20kd myosin light
chains. The relaxation of smooth muscle is mediated by the Endothelium-derived
relaxing factor-nitric oxide, endothelial derived hyperpolarizing factor (either
an endogenous cannabinoid, cytochrome P450 metabolite, or hydrogen peroxide),
or prostacyclin (PGI2). Nitric oxide and PGI2 stimulate soluble guanylate
cyclase and membrane bound adenylate cyclase, respectively. These cyclic
nucleotides activate Protein Kinase G and Proten Kinase A and phosphorylate a
number of proteins. The phosphorylation events lead to a decrease in
intracelluar calcium (inhibit L type Calcium channels, inhibits IP3 receptor
channels, stimulates sarcoplasmic reticulum Calcium pump ATPase), a decrease in
the 20kd myosin light chain phosphorylation by altering calcium sensitization
and increasing myosin light chain phosphatase activity, a stimulation of
calcium sensitive potassium channels which hyperpolarize the cell, and the phosphorylation
of amino acid residue serine 16 on the small heat shock protein (hsp20)by
Protein Kinases A and G. The phosphorylation of hsp20 appears to regulate actin
and focal adhesion dynamics, and recent evidence indicates that hsp20 binding
to 14-3-3 protein is envolved in this process. The endothelium derived
hyperpolarizing factor stimulates calcium sensitive potassium channels and/or
ATP sensitive potassium channels and stimulate potassium efflux which
hyperpolarizes the cell and produces relaxation. [edit]
Invertebrate Smooth Muscle In invertebrate smooth muscle, contraction is
initiated with calcium directly binding to myosin and then rapidly cycling
cross-bridges generating force. Similar to vertebrate smooth muscle there is a
low calcium and low energy utilization catch phase. This sustained phase or
catch phase has been attributed to a catch protein that has similarities to
myosin light chain kinase and the elastic protein-titin called twitchin.
Mollusk like clams use this catch phase of smooth muscle to keep their shell
closed for prolonged periods with little energy usage. [edit]
Control Smooth muscle cells can be stimulated to contract or relax in many
different ways. They may be directly stimulated by the autonomic
nervous system ("involuntarily" control),
but can also react on stimuli from neighbouring cells and on hormones (vasodilators or vasoconstrictor) within the
medium that it carries. [edit]
Growth and rearrangement The mechanism in which external factors stimulate
growth and rearrangement is not yet fully understood. A number of growth
factors and neurohumoral agents influence smooth muscle growth and
differentiation. The Notch receptor and cell signalling pathway has been
demonstrated to be essential to vasculogenesis and the formation of arteries and
veins. The embryological origin of smooth muscle is usually of mesodermal
origin. However, the smooth muscle within the Aorta and Pulmonary arteries (the
Great Arteries of the heart) is derived from ectomesenchyme of neural crest
origin, although coronary artery smooth muscle is of mesodermal origin. [edit]
Related diseases "Smooth muscle condition" is a condition in which
the body of a developing embryo does not create enough smooth muscle for the gastrointestinal
system. This condition is fatal.
Anti-smooth muscle antibodies (ASMA) can
be a symptom of an auto-immune
disorder, such as hepatitis,
cirrhosis, or lupus.
Vascular smooth muscle tumors are very rare. They can be malignant or benign,
and morbidity can be significant with either type. Intravascular leiomyomatosis
is a benign neoplasm that extends through the veins, angioleiomyoma is a benign
neoplasm of the extremities, vascular leiomyosarcomas is a malign neoplasm that
can be found in the inferior vena cava, pulmonary arteries and veins and other
peripheral vessels.
See Atherosclerosis.
Sphenoid bone
http://en.wikipedia.org/wiki/Sphenoidal_bone
http://www.bartleby.com/107/35.html
The sphenoid bone is situated at the
base of the skull in front of the temporalis and basilar part of the occipital.
It somewhat resembles a bat with its wings extended, and is divided into a
median portion or body, two great and two small wings extending outward from
the sides of the body, and two Pterygoid processes which project from it below.
Sphenobasilar (SB) junction [48]
[49]
The sphenoid articulates with the base
of the occipital bone to form the sphenobasilar (SB) junction, one of the most
vital articulations in the body. It serves as a “pump” (the sphenobasilar pump)
to move cerebrospinal fluid (CSF), which bathes the nervous system, delivering
nutrients, removing wastes and modulating the neuroimmune system.
Striated muscle (Skeletal muscle)
http://en.wikipedia.org/wiki/Skeletal_muscle
Muscle tissue that is marked by transverse
dark and light bands, is made up of elongated usually multinucleated fibers,
and includes skeletal muscle, cardiac muscle, and most muscle of arthropods. Skeletal
muscle is a type of striated
muscle, usually
attached to the skeleton.
Skeletal muscles are used to create movement, by applying force to bones
and joints; via contraction.
They generally contract voluntarily (via somatic nerve
stimulation), although they can contract involuntarily through reflexes. Muscle cells
(also called fibers) have an elongated, cylindrical
shape, and are multinucleated (in vertebrates
and flies). The nuclei
of these muscles are located in the peripheral aspect of the cell, just under
the plasma membrane,
which vacates the central part of the muscle fiber for myofibrils. (Conversely,
when the nucleus is located in the center it is considered a pathologic
condition known as centronuclear myopathy.)
Skeletal muscles have one end (the "origin") attached to a bone
closer to the centre of the body's axis and this is often but not always a
relatively stationary bone (such as the scapula) and the other
end (the "insertion") is attached across a joint
to another bone further from the body's axis (such as the humerus). Contraction
of the muscle causes the bones to rotate about the joint and the bones to move
relative to one another (such as lifting of the upper arm in the case of the
origin and insertion described here). There are several different ways to
categorize the type of skeletal muscle. One method uses the type of protein
contained in myosin (one of the important proteins that is responsible for the
ability of muscle to contract). Using this classification scheme, there are two
major types of fibers for skeletal muscles: Type I and Type II. Type I fibers
appear reddish. They are good for endurance and are slow to tire because they
use oxidative
metabolism. Type II fibers are whitish; they are
used for short bursts of speed and power, and use both oxidative metabolism and
anaerobic
metabolism depending on the particular sub-type,
and are therefore quicker to tire. How skeletal muscle works Main article: Muscle
contraction Bodybuilder demonstrating highly
developed skeletal muscle. The strength of skeletal muscle is directly
proportional to its length and cross-sectional area.
The strength of a joint, however, is determined by a number of biomechanical principles,
including the distance between muscle insertions and pivot points and muscle
size. Muscles are normally arranged in opposition so that as one group of
muscles contract, another group 'relaxes' (in fact simply stretched) or
lengthens. Antagonism in the transmission of nerve impulses (epsp and ipsp
balance) to the muscles means that it is impossible to stimulate the
contraction of two antagonistic muscles at any one time. During ballistic
motions such as throwing, the antagonist muscles act to 'brake' the agonist
muscles throughout the contraction, particularly at the end of the motion. In
the example of throwing, the chest and front of the shoulder
(anterior Deltoid) contract to pull the arm forward, while the muscles in the back
and rear of the shoulder (posterior Deltoid) also contract and undergo eccentric
contraction to slow the motion down to avoid
injury. Part of the training process is learning to relax the antagonist
muscles to increase the force output of the chest and anterior shoulder.
Skeletal muscle cells are stimulated by acetylcholine, which is
released at neuromuscular
junctions by motor neurons.[1] Once the cells
are "excited", their sarcoplasmic
reticulums will release ionic
calcium (Ca2+),
this interacts with the myofibrils and induces muscular contraction (via the sliding filament
mechanism). Besides calcium, this process
requires adenosine
triphosphate (ATP). The ATP is produced by metabolizing creatine
phosphate and glycogen within the
muscle cells by mitochondria,
as well by metabolizing glucose
and fatty acids, obtained from blood
and within the cell. Each motor neuron activates a group of muscle cells, and
collectively the neurons and muscle cells are known as motor units. When more strength is required
than can be obtained from a single motor unit, more units will be stimulated;
this is known as motor unit
recruitment. If more strength is required than can
be obtained from the current degree of unit contraction, the motor neurons
continue to recruit more motor units, and increase the frequency of neuronal
firing. This results in tetanic
contraction, which causes maximal muscular
contraction. [edit]
Red and white fibers Skeletal muscles contain two main types of fibers, which
differ in the mechanism they use to produce ATP; the amount of each type of
fiber varies from muscle to muscle and from person to person. Red
("slow-twitch") fibers have more mitochondria, store oxygen
in myoglobin, rely on aerobic
metabolism, have a greater capillary to volume ratio
and are associated with endurance;
these produce ATP more slowly. Marathon runners
tend to have more red fibers, generally through a combination of genetics and
training. White ("fast-twitch") fibers have fewer mitochondria, are
capable of more powerful (but shorter) contractions, metabolize ATP more
quickly, have a lower capillary to volume ratio, and are more likely to
accumulate lactic acid.
Weightlifters
and sprinters tend to have
more white fibers. Fast fibers come in three varieties, called type IIa, IIx
and IIb. Type IIx fibers in people used to be called, confusingly, type IIB.
Type IIb fibers predominate in the fast muscle of small mammals that have to
accelerate their limbs very fast against little load. Human type IIx (aka IIB)
are our fastest fibers. Type IIc fibers are the slowest of all of them, and
have only 36 units of myosin.[citation
needed] [edit]
Characteristics of muscle types
|
Fiber Type |
Type I fibers |
Type II a fibers |
Type II x fibers |
Type II b fibers |
|
Contraction time |
Slow |
Moderately Fast |
Fast |
Very fast |
|
Size of motor neuron |
Small |
Medium |
Large |
Very large |
|
Resistance to fatigue |
High |
Fairly high |
Intermediate |
Low |
|
Activity Used for |
Aerobic |
Long-term anaerobic |
Short-term anaerobic |
Short-term anaerobic |
|
Maximum duration of use |
Hours |
<30 minutes |
<5 minutes |
<1 minute |
|
Force production |
Low |
Medium |
High |
Very high |
|
Mitochondrial density |
High |
High |
Medium |
Low |
|
Capillary density |
High |
Intermediate |
Low |
Low |
|
Oxidative capacity |
High |
High |
Intermediate |
Low |
|
Glycolytic capacity |
Low |
High |
High |
High |
|
Major storage fuel |
Creatine phosphate, glycogen |
Creatine phosphate, glycogen |
[edit] Genes that define
skeletal muscle phenotype Skeletal muscle fiber-type phenotype in adult
animals, and probably people, is regulated by several independent signaling
pathways. These include pathways involved with the Ras/mitogen-activated
protein kinase (MAPK), calcineurin, calcium/calmodulin-dependent protein kinase
IV, and the peroxisome proliferator γ coactivator 1 (PGC-1). The Ras/MAPK
signaling pathway links the motor neurons and signaling systems, coupling
excitation and transcription regulation to promote the nerve-dependent
induction of the slow program in regenerating muscle. Calcineurin, a
Ca2+/calmodulin-activated phosphatase implicated in nerve activity-dependent
fiber-type specification in skeletal muscle, directly controls the
phosphorylation state of the transcription factor NFAT, allowing for its
translocation to the nucleus and leading to the activation of slow-type muscle
proteins in cooperation with myocyte enhancer factor 2 (MEF2) proteins and
other regulatory proteins. Calcium-dependent Ca2+/calmodulin kinase activity is
also upregulated by slow motor neuron activity, possibly because it amplifies
the slow-type calcineurin-generated responses by promoting MEF2 transactivator
functions and enhancing oxidative capacity through stimulation of mitochondrial
biogenesis.
Contraction-induced changes in
intracellular calcium or reactive oxygen species provide signals to diverse
pathways that include the MAPKs, calcineurin and calcium/calmodulin-dependent
protein kinase IV to activate transcription factors that regulate gene
expression and enzyme activity in skeletal muscle.

![]()
Exercise-Included Signaling Pathways in
Skeletal Muscle That Determine Specialized Characteristics of ST and FT Muscle
Fibers PGC1-α, a transcriptional coactivator of nuclear receptors
important to the regulation of a number of mitochondrial genes involved in
oxidative metabolism, directly interacts with MEF2 to synergistically activate
selective ST muscle genes and also serves as a target for calcineurin
signaling. A peroxisome proliferator-activated receptor δ
(PPARδ)-mediated transcriptional pathway is involved in the regulation of
the skeletal musclefiber phenotype. Mice that harbor an activated form of PPARd
display an “endurance” phenotype, with a coordinated increase in oxidative enzymes
and mitochondrial biogenesis and an increased proportion of ST fibers.
Thus—through functional genomics—calcineurin, calmodulin-dependent kinase,
PGC-1α, and activated PPARδ form the basis of a signaling network
that controls skeletal muscle fiber-type transformation and metabolic profiles
that protect against insulin resistance and obesity. The transition from
aerobic to anaerobic metabolism during intense work requires that several
systems are rapidly activated to ensure a constant supply of ATP for the
working muscles. These include a switch from fat-based to carbohydrate-based
fuels, a redistribution of blood flow from nonworking to exercising muscles,
and the removal of several of the byproducts of anaerobic metabolism, such as
carbon dioxide and lactic acid. Some of these responses are governed by
transcriptional control of the FT glycolytic phenotype. For example, skeletal
muscle reprogramming from a ST glycolytic phenotype to a FT glycolytic
phenotype involves the Six1/Eya1 complex, composed of members of the Six
protein family. Moreover, the Hypoxia Inducible Factor-1α (HIF-1α)
has been identified as a master regulator for the expression of genes involved
in essential hypoxic responses that maintain ATP levels in cells. Ablation of
HIF-1α in skeletal muscle was associated with an increase in the activity
of bob-limiting enzymes of the mitochondria, indicating that the citric acid
cycle and increased fatty acid oxidation may be compensating for decreased flow
through the glycolytic pathway in these animals. However, hypoxia-mediated
HIF-1α responses are also linked to the regulation of mitochondrial
dysfunction through the formation of excessive reactive oxygen species in
mitochondria. Other pathways also influence adult muscle character. For example,
physical force inside a muscle fiber may release the transcription factor Serum
Response Factor (SRF) from the structural protein titin, leading to altered
muscle growth.
Sympathetic ganglion
http://en.wikipedia.org/wiki/Sympathetic_ganglia
Sympathetic ganglia
are the ganglia
of the sympathetic
nervous system. They deliver information to the
body about stress
and impending danger, and are responsible for the familiar fight-or-flight
response. They contain approximately 20000–30000
nerve cell bodies and are located close to and either side of the spinal cord
in long chains. The bilaterally symmetric sympathetic
chain ganglia, also called the paravertebral
ganglia, are located just anterior and lateral to the spinal cord. The chain
extends from the upper neck down to the coccyx,
forming the unpaired coccygeal
ganglion. Preganglionic nerves from the spinal cord synapse at one of the
chain ganglia and the postganglionic fiber extends to an effector, typically a visceral organ in the thoracic cavity. Neurons of the
collateral
ganglia, also called the prevertebral
ganglia, receive input from the splanchnic nerves and innervate
organs of the abdominal
and pelvic region. These
include the celiac ganglia,
superior
mesenteric ganglia, and inferior
mesenteric ganglia.
http://en.wikipedia.org/wiki/Sympathetic_nervous_system
The Sympathetic Nervous System (SNS)
is a branch of the autonomic
nervous system. It is always active at a basal
level (called sympathetic tone) and becomes more active during times of stress.
Its actions during the stress response comprise the fight-or-flight
response. Like other parts of the nervous system, the
sympathetic nervous system operates through a series of interconnected neurons.
Sympathetic neurons are frequently considered part of the peripheral
nervous system (PNS), although there are many
that lie within the central nervous
system (CNS). Sympathetic neurons of the spinal cord (which is part
of the CNS) communicate with peripheral sympathetic neurons via a series of sympathetic
ganglia. Within the ganglia, spinal cord
sympathetic neurons join peripheral sympathetic neurons through chemical synapses. Spinal cord
sympathetic neurons are therefore called presynaptic (or preganglionic)
neurons, while peripheral sympathetic neurons are called postsynaptic
(or postganglionic) neurons. At synapses within the sympathetic ganglia,
preganglionic sympathetic neurons release acetylcholine, a chemical
messenger that binds and activates nicotinic
acetylcholine receptors on postganglionic
neurons. In response to this stimulus, postganglionic neurons principally release
noradrenaline
(norepinephrine).
Prolonged activation can elicit the release of adrenaline from the adrenal medulla. Once released,
noradrenaline and adrenaline bind adrenergic
receptors on peripheral tissues. Binding to
adrenergic receptors causes the effects seen during the fight-or-flight
response. These include pupil dilation, increased sweating, increased heart
rate, and increased blood pressure.
Thermoreceptors
Detect changes in temperature
Thoracic splanchnic nerves
http://en.wikipedia.org/wiki/Thoracic_splanchnic_nerves
http://en.wikipedia.org/wiki/Image:Gray838.png
{kind=link}
Thoracic splanchnic nerves
arise from the sympathetic trunk
in the thorax and travel
inferiorly to provide sympathetic innervation to the abdomen. The nerves
contain preganglionic
sympathetic and visceral afferent fibers. There
are three main thoracic splanchnic nerves: greater[1]= T5-T9[2] or T5-T10[3]= The nerve
travels through the diaphragm
and enters the abdominal cavity, where its fibers synapse at the celiac ganglia. The nerve
contributes to the celiac plexus,
a network of nerves located in the vicinity of where the celiac trunk branches from
the abdominal aorta.
The fibers in this nerve modulate the activity of the enteric nervous
system of the foregut. They also provide
the sympathetic innervation to the adrenal medulla, stimulating catecholamine release. lesser[4]= T9-T12, T9-T10[4][5], T10-T12, or
T10-T11[3]= The nerve
travels inferiorly, lateral to the greater splanchnic nerve. Its fibers synapse
with their postganglionic counterparts in the celiac ganglia, or in the aorticorenal
ganglion. The nerve modulates the activity of
the enteric nervous system of the midgut.
least or lowest[6]= T12-L2, or
T11-T12[7]= The nerve
travels into the abdomen, where its fibers synapse in the renal ganglia.
http://members.telering.at/pfs/gordon.htm
World-renowned psychologist, Dr. Thomas Gordon,
author of Parent Effectiveness Training (P.E.T.) and founder of Gordon Training
International of Solana Beach, California, died Monday, August 26, after a bout
with prostate cancer. He was 84. Dr. Gordon spent more than 50 years teaching
parents, teachers and leaders the model he developed for building effective
relationships. His model was based on a strong belief that the use of coercive
power damages relationships. As an alternative, he taught people skills for
communicating and resolving conflicts that they can use to build and maintain
good relationships at home, school and at work. These skills, which include
Active Listening, I-Messages and No-Lose Conflict Resolution, are now widely
known and used by people around the world. Dr. Gordon first applied some of
these methods in the 1950s as a consultant to business organizations. Then, in
the early 60s, he developed the Parent Effectiveness Training course—commonly
known as P.E.T.—and taught the first class to a group of 14 parents in a
Pasadena, CA cafeteria. The courses proved to be so popular with parents that
he began training instructors throughout the U.S. to teach it in their
communities. Over the next several years, the course spread to all 50 states.
http://en.wikipedia.org/wiki/Unconditional_positive_regard
Unconditional positive regard (UPR) is a
concept in client-centered therapy. Carl Rogers, who created client-centered
therapy, designated unconditional positive regard as one of the three
conditions were necessary for positive change, along with empathy and
genuineness (congruence). Unconditional positive regard encourages the
therapist, termed a counselor by Rogers, to treat the client as worthy and
capable, even when the client does not act or feel that way. According to the
Rogers's theory, mental illness is often caused by the absence of love, or by a
defective kind of love, that the client received as a child. By showing the client
unconditional positive regard and acceptance, the therapist is providing the
best possible conditions for personal growth to the client. To practice
unconditional positive regard, while maintaining congruence at all times, the
therapist provides specific feedback. The counselors show and demonstrate their
care with their actions. If a clinician finds it hard to unconditionally regard
their patient in a positive light, they need to keep in mind Rogers’ belief
that all people have the internal resources required for personal growth.
According to this theory, it is the environment that can make the difference as
to whether growth occurs. A patient’s past environment may have been such that
patterns of behaviour were developed in order to survive in that environment.
These patterns can become entrenched so that the patient continues to operate
in the world with them even if they are no longer appropriate. It is usually an
inappropriate pattern that makes it hard for the clinician to regard their
clients positively. The clinician needs to feel for the person under those
patterns and for the person who was damaged and then survived by adapting by
developing the patterns that are no longer appropriate. Unconditional positive
regard has been described as the opposite of unconditional negative disgust, a
term coined by therapist- Matt Vaughn
http://en.wikipedia.org/wiki/Vagus_nerve
The vagus nerve (also called pneumogastric
nerve or cranial nerve X) is the tenth of twelve paired cranial nerves, and is the
only nerve that starts in the brainstem (within the medulla oblongata) and extends,
through the jugular foramen,
down below the head,
to the neck, chest and abdomen.
The medieval Latin
word vagus means literally "Wandering" (the words vagrant, vagabond, and vague come from the
same root). It is also called the pneumogastric nerve since it
innervates both the lungs and the stomach. The vagus nerve supplies motor parasympathetic fibers to all
the organs except the suprarenal (adrenal) glands, from
the neck down to the second
segment of the transverse colon.
The vagus also controls a few skeletal muscles
Viscera
http://en.wikipedia.org/wiki/Viscera
In anatomy, a viscus (plural: viscera)
is an internal organ of an animal (including humans), in particular an internal
organ of the thorax or abdomen. The viscera, when removed from a butchered
animal, are known collectively as offal. Internal organs are also known as
"innards", or less formally, "guts" (which may also refer
to the gastrointestinal tract). The adjective visceral is used for anything
pertaining to the internal organs. Historically, viscera of animals were
examined by Roman pagan priests like the haruspices or the augurs in order to
divine the future by their shape, dimensions or other factors.
Visceroceptors (Enteroceptors)
Provide information about the internal
environment. These sensations arise from within the body and may be felt as
pain, pressure, fatique, hunger, thirst and nausea. Visceroceptors are located
in blood vessels and viscera.
ENDNOTES