Journal Club Activities
Copyright © December 2006 Ted Nissen
TABLE OF
CONTENTS
1 November 2006
1.1.1 Group Discussion
Questions
1.1.1.1
November Articles
1.1.1.1.1 What was the funding source
for this research project?
1.1.1.1.2 Did the people in the study
as a whole have a significantly impaired lumbar range of motion pre-treatment?
Was it within the normal range?
1.1.1.1.3 Did the comprehensive
massage therapy group (Group # 1) have significantly improved scores at
follow-up compared with the soft-tissue manipulation group (Group # 2)?
1.1.1.1.3.1
http://www.anatomyfacts.com/Research/Massage%20Journal%20Club/November06/novemberAnal06.htm#results
1.1.1.1.4 Were subjects and or
therapists/PTs/Trainers paid and if so how much?
1.1.1.1.5 Can we get charts and other
ancillary material depicting/describing stretches/postural education massage
techniques used?
1.1.1.1.6 Would
the less expensive form of massage therapy (Is there a less expensive version
in Canada) performed by non-registered therapists be as effective as the $50
version performed by registered massage therapists?
1.1.1.1.7 Would
untrained unregistered massage therapists produce similar results?
1.1.1.1.8 How much did this research
cost?
1.1.1.1.9 Given
that the author agrees this would have been a better control treatment how much
more would sham massage have cost to do?
1.1.1.1.10 Is
blinding therapists, subjects, and assessors more expensive and time consuming
in a research project? If so how much?
1.1.1.1.11 Was
there a time constraint to the research?
1.1.1.1.12 Despite
the fact that the providers of both the sham laser and exercise treatment
groups believed that the exercise to be an effective remedy, at posttest 8% of
the subjects in the sham laser group indicated that they had no pain as
compared with 5% in the exercise and education group. Does this mean that
blinding therapists in this experiment would have no effect on the reported
treatment effects of subjects? Have other studies been done about the effect of
therapists expectations on the self-reporting behavior of subjects?
1.1.1.1.13 What
other research studies have followed this one and have added to our knowledge
of subacute (falling between acute and chronic in character especially when
closer to acute less marked in severity or duration than a corresponding acute
state) low-back pain?
1.1.1.1.14 Doesn’t
the fact that there was no improvement in actual function (range of motion test
(Schober)) invalidate the results of the Roland Disability Questionnaire (RDQ),
which relies on patient assessment? How well researched is the RDQ score?
1.1.1.1.15 How well are the self-rated
measures (RDQ, PRI & PPI, state anxiety) researched for reliability,
validity and internal consistency?
1.1.1.1.16 Isn’t
one person’s rating for intensity of pain (PPI) for example different from
another persons? Perhaps the same person may even rate the pain differently on
different days? Aren’t these self-rating numbers based on a nominal scale (Scales) which
although indicate greater and or less than values have indeterminate intervals
between numbers and therefore defy statistical analysis?
1.1.1.1.17 Wouldn’t
a better research design just have done away with the self-rating tests and
just used objective measures with blinded assessors?
1.1.1.1.18 Why
was Analgesic use permitted?
1.1.1.1.19 Are
Self-reported criteria (past history info) are unreliable?
1.1.1.1.20 Subjects
were told in the advertisements they might receive "one or more
modalities" This according to Preyde might dilute their expectations.
Expectations of what? That comprehensive massage was the therapeutic treatment.
1.1.1.1.21 According
to Preyde each group had approximately the same dropout rate (1 or 2 per group)
What does this have to do with Oppel & Sedergreen comments?
1.1.1.1.22 Is
it true as Preyde states that no study has employed a truly objective measure
of subacute back pain (e.g., laboratory investigations)
1.1.1.1.23 Preyde
states that history taking and physical examination (was this by a physician
other than the subjects physician) helped rule out both contraindications to
massage therapy as well as exclusion criteria. She seems to be implying a
greater physicians role than was apparent in the research. Was there a greater
physicians role?
1.1.1.1.24 Preyde
doesn’t think ancillary tests are appropriate. I assume she is referring to
ruling out cancer. Can't be sure cause this passage is vague. But she does cite
the following research.[1]
Is Preyde referring to cancer?
1.1.1.1.25 Should medication use have
been prohibited of subjects for this study?
1.1.1.1.26 The author makes two
references in her research article to the use of a registered massage
therapist, why was this important when this factor (training level of
therapist) was not being tested? (the specific techniques of soft tissue
mobilization; friction, trigger point therapy, and neuromuscular therapy were
the independent variables) First the author cites the fault of previous
research in not using registered therapists [2] Second the authors cites her
own use of registered massage therapists in research and her own status as a
registered massage therapist [3] Are there studies to
indicate that registered massage therapists result in improved treatment
results? The author has an affiliation with the College of Massage Therapists of Ontario which has
as its mission statement "All qualified massage therapists are registered
and proud to be associated with the College" In her summary conclusion the
author states "Patients with subacute low-back pain were shown to benefit
from massage therapy, as regulated by the College of Massage Therapists of
Ontario and delivered by experienced massage therapists." [4] Were the registered massage
therapists in this research study registered by the College of Massage
therapists? Similar emphasis of place of educational certification was not placed
on the other providers of treatment in this research study e.g. personal
trainer, weight-trainer supervisor & physiotherapists. We do not learn for
example that their training/registration/certification/schooling benefited the
outcome of the research. Is there bias in this research which may have been
transmitted to the subjects (subjects use self-rating of pain and function
which may be influenced by therapeutic bias) by the proud registered massage
therapy providers (the author included) who at least in the case of the author
were a member of the college of massage therapists?
1.1.1.1.27 How
can Group 1 be statistically superior to group 3 since there are no reported
statistical differences between group 1 and group 2?
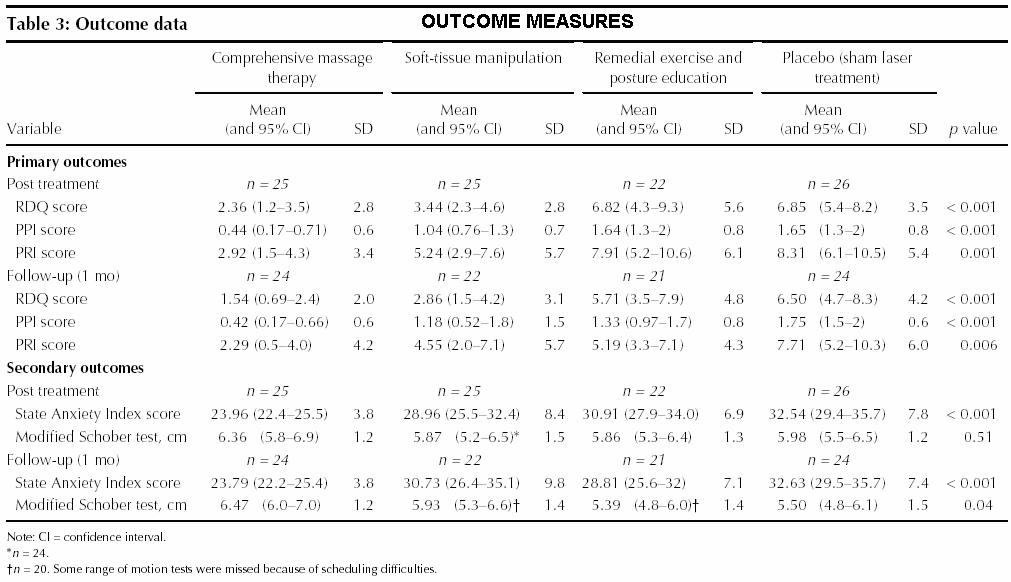
1.1.1.1.28 Was
there a significant difference between the means of the Lumbar range of motion
(ROM) (Schober) of the 4 groups? The P-Values
listed in Table 3 (Outcome
Measures) of the research paper are .04 which being less
than a significance level of .05 indicates significant difference between
groups. Why did the author not report this? What is the meaning of this
difference?
{kind=link}
1.1.2 Group Activities
November Article
1.1.2.1
Use the assessment tools of the November research article.
1.1.2.1.1 References
1.1.2.1.1.1
November Articles
1.1.2.1.1.2
Outcome Assessment-November Article
Analysis
1.1.2.1.2
Roland
Disability Questionnaire (RDQ)
1.1.2.1.2.1
Introduction/Instructions
1.1.2.1.2.1.1 The Roland Disability Questionnaire (RDQ) (AKA Roland-Morris Questionnaire (RMQ)) uses a 24-point scale. The test asks the patient to check off the functional limitations imposed by back pain that the client feels TODAY. The greater the number of items checked by the patient the greater the disability. Improvement can be calculated as a percentage of the total number of disabling attributes before and after a series of treatments. If, for example, at the beginning of treatment, a patient’s score was 12 and, at the conclusion of treatment, her/his score was 2 (10 points of improvement), we would calculate an 83% improvement. (10/12=83%).
1.1.2.1.2.1.2 Place the total score in the box on the bottom left of the form and the percentage improvement in the box on the bottom right of the form.
1.1.2.1.2.1.3 In terms of point increases/decreases a change of 2.5 points or greater considered clinically significant.
1.1.2.1.2.1.4 Some practitioners have inserted back pain and/or leg pain. This is because sometimes clients don’t feel pain in their back but rather in the legs referred from the nerve root, which emanates from the lower lumbar vertebrae. The problem (nerve root irritation) is still a problem in the low back. This practice may more accurately reflect a client’s disability but has not as yet been validated as a disability test.
1.1.2.1.2.2
Test
1.1.2.1.2.2.1 http://www.anatomyfacts.com/research/roland.pdf
1.1.2.1.3
McGill
Pain Questionnaire (PPI and PRI)
1.1.2.1.3.1
Introduction
1.1.2.1.3.1.1 The Long version of this form was used in the November Research Study and the short form is included for your convenience. Both forms are well correlated with one another.
1.1.2.1.3.2
Short Form
(This was not used in the November research article but is research validated.)
1.1.2.1.3.3
1.1.2.1.3.3.1 Introduction/Instructions
1.1.2.1.3.3.1.1 Developed in the 1980’s assesses the quality of pain with both sensory (S-PRI) and affective (A-PRI) measures. The intensity of pain is assessed using a visual analog scale and a numbered (0-5) ordinal list (PPI).
1.1.2.1.3.3.1.2 Each sensory and affective pain quality is rated on a 0-3 scale where each number is characterized by a descriptor (0=None, 1=Mild, 2=Moderate, 3=Severe).
1.1.2.1.3.3.1.3 Subjects are asked to limit their pain to the pelvic region only while rating each of the pain qualities with a number between 0-3. Once completed the tester computes and marks the score for the S-PRI & A-PRI and adds the total of these scores into the T-PRI (Total Pain Rating Index) Box.
1.1.2.1.3.3.1.4
1.1.2.1.3.3.2 Test
1.1.2.1.3.3.2.1 http://www.anatomyfacts.com/research/mcgill.pdf
1.1.2.1.3.4
Long Form (This was used in the November Research
article)
1.1.2.1.3.4.1 Introduction/Instructions
1.1.2.1.3.4.1.1 Developed in the 1970’s
1.1.2.1.3.4.2 Test
1.1.2.1.3.4.2.1 http://www.anatomyfacts.com/research/mcgill2.pdf
1.1.2.1.4
State Anxiety Index
1.1.2.1.4.1
Need to get a copy
1.1.2.1.4.2
Reference (You can pay for a copy of this test at
this web site)
1.1.2.1.4.2.1 http://www.mindgarden.com/products/staisad.htm
1.1.2.1.5
Modified Schober test (lumbar range of motion) [5]
[6]
1.1.2.1.5.1
The modified Schober method: a technique for
assessing spinal motion. Although the technique is reliable (Moll & Wright,
1971), its primary usefulness may be in screening for the very limited mobility
that patients exhibit who have diseases like ankylosing spondylitis.
1.1.2.1.5.2
Use a pen to mark the midpoint between the
posterior superior iliac spines (PSIS). Then use your tape measure to identify
and mark two points: (1) one that is 10 cm superior to the PSIS, and (2) one
that is 5 cm inferior to the PSIS.
1.1.2.1.5.3
As the client flexes the spine as far as possible,
measure and record the distance between the superior and inferior marks.
1.1.2.1.5.4
Similarly, measure and record the distance between
the superior and inferior marks as your partner extends the spine as far as
possible.
1.1.2.1.5.5
This modification of the Schober test is published
in the following. [7] [8]
1.1.2.1.5.6
Test (Printable Form)
1.1.2.1.5.6.1 http://www.anatomyfacts.com/research/schober.pdf
1.1.2.1.5.7
Reference
1.1.2.1.5.7.1 http://moon.ouhsc.edu/dthompso/namics/labs/standing.htm
1.1.2.1.5.7.2
High
Tech Solutions
1.1.2.1.5.8
Pocket
PC/Mobile phone access to the assessment tools described above.
1.1.2.1.5.8.1 Instructions
1.1.2.1.5.8.1.1 If you have a pocket pc or mobile phone you can assess pdf files just like on your computer. First sync your pocket pc or mobile phone with your computer and download the appropriate version of Adobe Reader for mobile devices. The following is a adobe program download link.
1.1.2.1.5.8.1.1.1 http://www.adobe.com/products/acrobat/readstep2_mobile.html
1.1.2.1.5.8.1.2 Once the adobe software is installed into your mobile device upload the following files
1.1.2.1.5.8.2 http://www.anatomyfacts.com/research/pocketa.pdf
1.1.2.2 Try these
Treatment Modalities Outlined in the November Article
1.1.2.2.1
Soft-tissue manipulation techniques
1.1.2.2.1.1
Purpose
1.1.2.2.1.1.1 Promote Circulation
1.1.2.2.1.1.2 Relax Muscle Spasm
1.1.2.2.1.2
Procedure
1.1.2.2.1.2.1 Subjects were asked to identify the area that was bothering them. The appropriate technique was used for that area according to the criterion below.
1.1.2.2.1.3
Duration
1.1.2.2.1.3.1 30 and 35 minutes
1.1.2.2.1.4
Frequency
1.1.2.2.1.4.1 Six treatments over a one month period
1.1.2.2.1.5
Friction (Used for Fibrous Tissue)
1.1.2.2.1.6
Trigger points (Muscle Spasm)
1.1.2.2.1.7
Neuromuscular therapy
1.1.2.2.2 Exercise/Postural Correction
1.1.2.2.2.1
Initial
Session
1.1.2.2.2.1.1 Exercise instruction demonstrates stretching exercises for the trunk, hips and thighs, including flexion and modified extension
1.1.2.2.2.1.2 Stretches to be performed in a relaxed manner within the pain free range held for 30 seconds
1.1.2.2.2.1.3 Subjects instructed to perform stretches twice one time per day for related areas and more frequently for affected areas
1.1.2.2.2.1.4 Subjects encouraged to engage in strengthening or mobility exercises such as walking, swimming or aerobics and to build overall fitness progressively
1.1.2.2.2.1.5 Subjects were given postural education and proper body mechanics instruction, particularly as they related to work and daily activities
1.1.2.2.2.2
Each subsequent session
1.1.2.2.2.2.1 Includes stretching exercises with review of proper mechanics, postural education and reinforcement of home practice and ancillary exercise activities
1.1.2.2.2.3
Duration
1.1.2.2.2.3.1 15-20 Minutes with therapist
1.1.2.2.2.3.2 Self exercise 1 x per day 2 repetitions= 15- 20 minutes (?).