November Article Analysis
Copyright © December 2006 Ted Nissen
TABLE OF CONTENTS
3.1 Research Literacy (Summary of
Concepts)
3.2 Baseline Data (Initial
pre-treatment measures)
1
Research Article Links
1.1.1 http://www.anatomyfacts.com/Research/blog.htm
2
Analysis
2.1 Brief Summary
2.1.1 This is a novel, randomized (Alternate Definition-Random Sample),
and controlled research study (a study using a (control group) on comprehensive massage therapy combining soft tissue manipulation
(trigger point, neuromuscular, and friction) with exercise/ postural correction
in the treatment of subacute low back pain. The comprehensive massage group
is compared with 3 other groups; soft tissue only group, exercise/postural
group, and control group (fake laser treatments=The laser machine was not
working-this was a control group) (GROUPS). The
comprehensive massage group does no better than the soft tissue only group,
which is in a statistical dead heat (There was no difference between the
treatments-that is the clients got about the same benefit from either
treatment) with the exercise group at one-month follow-up. All of the 3
treatment groups do better than the fake laser group. Consumers would be
advised to pick the treatment based on time and cost. The least time consuming option for clients
would be soft tissue treatment and the least expensive would be
exercise/postural correction. The comprehensive massage therapy may provide
better pain relief (although potential bias and questionable statistics makes
for an uncertain result) but is both more expensive and time consuming than the
other alternatives.
2.2 Effectiveness of massage therapy for subacute low-back pain: a
randomized controlled trial By Michele Preyde
2.2.1 Introduction
2.2.1.1
This Peer reviewed [1] article is according to its author, Michele Preyde "the first
randomized controlled trial of the effectiveness of massage therapy for
subacute low-back pain." [2]
Randomizing insures that researches can't pick clients that will prove their
point and control groups allow researches to compare different treatments one
with the other and with no treatment. This is a way to measure the
effectiveness of treatment. This research would probably be considered more
valid by statistical/research design type people because it follows good,
acceptable scientific method.
2.2.1.2
Nearly 100 people, mostly
overweight, college educated women in their mid to late 40’s, who had chronic
low back pain (1 week-8 months) (from bending or lifting), without significant
pathology (No serious disease of the lumbar spine or other serious diseases,
diabetes, Multiple Sclerosis ect) completed the study. The large numbers of
clients treated means the statistics are more accurate because this is a large
sample. This study would have as they say street credibility (street creds), if
your street is a research lab and your audience were research scientists.
2.2.2 Research Validity
2.2.2.1
Pedro rates this research as
follows; 6 out of 10 possible (see Pedro Validity Standards). This
study did have some significant flaws which are outlined below.
2.2.2.1.1 “6/10
[Eligibility criteria: Yes; Random Allocation: Yes; Concealed Allocation:
No; Baseline comparability: Yes; Blind Subjects: No; Blind Therapists: No; Blind Assessors: Yes; Adequate follow-up: Yes; Intention to treat: No; Between-group comparisons:
Yes; Point estimates and variability: Yes. Note: Eligibility criteria item does
not contribute to total score] * This score has been confirmed*” Pedro
2.2.2.2
Analysis of Weaknesses in this
Research
2.2.2.2.1 Had
the following criterion been met this research study would have gotten a
perfect score of 10. The following attempts to explain the criterions, which
were not met by this research study.
2.2.2.2.2
Concealed Allocation [3]
2.2.2.2.2.1 This
study does not clarify whether or not the screening person was unaware of which
group the subject would be placed in. The screening person determines if a
subject is eligible as participant in the research Allocation assignments, for
example, should be sealed (opaque envelopes) to the screening person or
allocation should be done by a person “off-site” to the research project, and
by someone who has no association to the project personal. This would insure
that the screening person’s bias did not influence which subjects were placed
in what groups.
2.2.2.2.2.2 When
allocation is concealed from the researcher some studies (Schulz et al. (1995),
JAMA 273(5): 408-412)) show more modest treatment effects. This can in effect
reduce or nullify the positive effects of randomization in reducing researcher
bias so that it has minimal effect on outcome. [4]
2.2.2.2.2.3 In
this study people were assigned randomly using a random number table what is not clear is whether the
allocation person knew who was being assigned to which groups.
2.2.2.2.2.4
2.2.2.2.2.5 Reference
2.2.2.2.2.5.1 http://www.anatomyfacts.com/Research/allocationc.pdf
2.2.2.2.2.5.2 http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=11867132
2.2.2.2.3
Blind Subjects
2.2.2.2.3.1 This research did not insure
that subjects in the study were unaware of whether they had received treatment.
If subjects can’t be sure whether they received treatment it is less likely
they will be influenced by Placebo Effects Hawthorne effects or Observer Effect.
2.2.2.2.4
Blind Therapists
2.2.2.2.4.1 The
therapists in this study were aware of which groups they were treating and
therefore were not blinded. Since one of the therapists had a family emergency
the researcher who was also a registered massage therapist provided treatment
thus raising questions about Experimenter's Bias.
2.2.2.2.5
Intention to treat
2.2.2.2.5.1 In
this study all of the subjects scores who were intended for treatment were not
statistically analyzed together. If subjects dropped out or did not complete
all of the treatments their scores were dropped from the statistical pool. This
can reverse the good effects of randomization in eliminating bias according to
some research. [5] [6]
It can result in an increasing the probability of what is known as Type 1 Error, which involves
rejecting the null hypothesis when it should be accepted. Research usually
begins with a Null Hypothesis, which is a
statement that predicts the research will show no difference in the means
between the treatment groups and control groups. A hypothesis then is a
prediction about the outcome of the research. The null hypothesis predicts the
null (null=not any) effect of the treatment.
2.2.2.2.5.2 In this case when all of the
subjects scores even the ones that dropped out are not included it increases
the chance of rejecting the null hypothesis when it should be accepted. This
research may have shown treatment effects between the various groups when there
were none.
2.2.2.2.5.3 Reference
2.2.2.2.5.3.1
Statistical Considerations
2.2.2.2.5.3.2
http://www.bmj.com/cgi/content/short/319/7211/670
2.2.2.2.5.3.3
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=search&DB=pubmed
2.2.3 Treatment Setting
2.2.3.1
“This study was conducted at the
Health and Performance Centre, University of Guelph, Guelph, Ont., which offers
multidisciplinary services such as sports medicine, physiotherapy and
chiropractic manipulation. Treatments were provided and outcome measures were
obtained at this centre.” [7]
2.2.4 Screening and Random Assignment
2.2.4.1
Prospective subjects were
recruited via university E-Mail, flyers sent to family physicians and local
newspaper advertisements. Were subjects paid and if so how much? Telephone
screening of subjects (age range 18-81) determined the following;
2.2.4.1.1
Existence
of subacute (1 week-8 months) low-back pain
2.2.4.1.2
Absence
of significant pathology (bone fracture, nerve damage or severe psychiatric
condition (clinical depression as physician diagnosed)
2.2.4.1.3
No
pregnancy
2.2.4.1.4
Stable
health
2.2.4.1.5
Previous
episode of low-back pain ok
2.2.4.1.6
Positive
radiographic finding of mild pathology ok
2.2.4.2 Although the
information above was obtained as self-reported criteria along with their
information regarding health history. (Medical conditions, medication use past
history of serious injury) Doubts about a particular subjects inclusion in the
study were discussed with their personal physician.
2.2.4.3 Random assignment
using a random numbers table forming the 4 groups described below.
2.2.4.4 Upon the first
appointment the following was completed;
2.2.4.4.1
Patient
characteristics and health information
2.2.4.4.2
Informed
consent
2.2.4.4.3
Baseline
measures (Function, pain, anxiety and lumbar range of motion) were recorded
2.2.5 Modalities
2.2.5.1 Introduction
2.2.5.1.1 The
treatment consisted of several modalities, which were combined and labeled
comprehensive massage (Group # 1) by the researcher. Comprehensive massage
consisted of soft tissue mobilization, exercise, and postural education. These
modalities were also combined to form a total of 2 additional groups, which
were compared statistically to a Sham laser group (Total of 4 groups). (See below)
Subjects were also encouraged to increase their activity level between
treatment sessions
2.2.5.2 Soft-tissue manipulation techniques
2.2.5.2.1
Purpose
2.2.5.2.1.1
Promote Circulation
2.2.5.2.1.2
Relax Muscle Spasm
2.2.5.2.2
Procedure
2.2.5.2.2.1
Subjects
were asked to identify the area that was bothering them. The appropriate
technique was used for that area according to the criterion below.
2.2.5.2.3
Duration
2.2.5.2.3.1
30 and 35 minutes
2.2.5.2.4
Frequency
2.2.5.2.4.1
Six
treatments over a one month period
2.2.5.2.5
Friction (Used for Fibrous Tissue)
2.2.5.2.6
Trigger points (Muscle Spasm)
2.2.5.2.7
Neuromuscular therapy
2.2.5.3 Exercise/Postural
Correction
2.2.5.3.1
Initial
Session
2.2.5.3.1.1
Exercise
instruction demonstrates stretching exercises for the trunk, hips and thighs,
including flexion and modified extension
2.2.5.3.1.2
Stretches to be performed in a relaxed manner
within the pain free range held for 30 seconds
2.2.5.3.1.3
Subjects instructed to perform stretches twice one
time per day for related areas and more frequently for affected areas
2.2.5.3.1.4
Subjects encouraged to engage in strengthening or
mobility exercises such as walking, swimming or aerobics and to build overall
fitness progressively
2.2.5.3.1.5
Subjects were given postural education and proper
body mechanics instruction, particularly as they related to work and daily
activities
2.2.5.3.2
Each subsequent session
2.2.5.3.2.1
Includes stretching exercises with review of
proper mechanics, postural education and reinforcement of home practice and
ancillary exercise activities
2.2.5.3.3
Duration
2.2.5.3.3.1
15-20
Minutes with therapist
2.2.5.3.3.2
Self
exercise 1 x per day 2 repetitions= 15- 20 minutes (?).
2.2.5.4 Sham Laser Group
2.2.5.4.1
“The
control group received sham low-level laser (infrared) therapy. The laser was
set up to look as if it was functioning but was not. The subject was
"treated" lying on his or her side with proper support to permit
relaxation. The instrument was held on the area of complaint by the treatment
provider, so the subject was attended for the duration of the session (about 20
minutes) to control for the effects of interpersonal contact and support.” [8]
2.2.6 Modalities (Narrative from research)
2.2.6.1
“For subjects in the
comprehensive massage therapy group various soft-tissue manipulation techniques
such as friction, trigger points and neuromuscular therapy were used to promote
circulation and relaxation of spasm or tension. The exact soft tissue that the
subject described as the source of pain was located and treated with the
specific technique indicated for the specific condition of the soft tissue
(e.g., friction for fibrous tissue and gentle trigger points for muscle spasm).
The duration of the soft-tissue manipulation was between 30 and 35 minutes.
2.2.6.2
For each treatment, stretching
exercises for the trunk, hips and thighs, including flexion and modified
extension, were taught and reviewed to ensure proper mechanics. Stretches were
to be within a pain-free range, held for about 30 seconds in a relaxed manner,
and performed twice on one occasion per day for the related areas and more
frequently for the affected areas. Subjects were encouraged to engage in
general strengthening or mobility exercises such as walking, swimming or
aerobics and to build overall fitness progressively. Education of posture and
body mechanics, particularly as they related to work and daily activities, was provided.
The exercise and education segment took about 15-20 minutes.” “Each subject
received 6 treatments within approximately 1 month.” [9]
2.2.7 Groups
2.2.7.1
Subjects (clients) were placed
randomly in one of four groups.
2.2.7.2
Group # 1 Comprehensive massage
therapy
2.2.7.2.1 Soft-tissue
manipulation
2.2.7.2.2 Remedial
exercise
2.2.7.2.3 Posture
education
2.2.7.3
Group # 2 Soft Tissue Only
2.2.7.3.1 Soft-tissue
manipulation
2.2.7.4
Group # 3 Remedial
exercise/Posture education only
2.2.7.4.1 Remedial
exercise
2.2.7.4.2 Posture
education
2.2.7.5
Group # 4 Placebo
2.2.7.5.1 Sham
laser treatment
2.2.8 Initial and
Outcome Measurement
2.2.8.1
Outcomes were measured using
questionnaires, which are well researched to provide reliable results
(reliability, validity and internal consistency). These questionnaires measured
activities of Daily Living (ADL)(functionality) and pain. Secondary measures
were anxiety and lumbar range of motion. The anxiety test measures anxiety at
the moment the lumbar range of motion test was taken. Often people who suffer
pain will experience anxiety prior to movement in the direction of pain (?).
This is a way to initially measure and then compare post treatment anxiety
levels associated with movement.
2.2.8.2
Despite the fact that many of
these self-rating tests are well researched for validity (still used by many
researchers) mainstream science (Oppel) may be sceptical of non-objective functional
assessment. [10] [11]
[12]
[13]
For insurance purposes many carriers are increasingly demanding functional
capacity examination as necessary justification for payment.
2.2.8.3
References
2.2.8.3.1 Quantitative functional Capacity Evaluation: The Missing
Link to Outcomes Assessment
2.2.8.3.2 Functional Capacity Evaluation and Chiropractic Case
Management
2.2.8.3.3 Applying Outcomes Management into Clinical Practice
2.2.8.3.4 Proving the Existence of Chronic Pain
2.2.8.4
“Post-treatment measures were obtained after 1
month of treatment, and follow-up measures were obtained 1 month after
treatment ended.” [14]
2.2.8.4.1 Post-Treatment
Measures=After 6 treatments (1 Month)
2.2.8.4.2 Follow-up
Measures=1 month post treatment Termination.
2.2.8.5
Definitions
2.2.8.5.1 Test
Described
2.2.8.5.1.1
2.2.8.5.2 Usage
2.2.8.5.2.1
2.2.8.5.3 Reliability
2.2.8.5.3.1
Intra observer & inter observer reliability
2.2.8.5.3.2 Reliability
2.2.8.5.3.3
2.2.8.5.4 Validity
2.2.8.5.4.1 Validity
2.2.8.5.4.2
2.2.8.5.5 Sensitivity
2.2.8.5.5.1 Sensitivity
2.2.8.5.6 Internal
consistency
2.2.8.5.6.1 Internal consistency
2.2.8.6
Tests used
2.2.8.6.1
Roland Disability Questionnaire (RDQ) (AKA Roland-Morris
Questionnaire (RMQ) (2.5 or greater considered clinically
significant)
2.2.8.6.1.1 Test
2.2.8.6.1.1.1 http://www.anatomyfacts.com/research/roland.pdf
2.2.8.6.1.1.2 Adaptations
2.2.8.6.1.1.2.1 http://www.anatomyfacts.com/research/roland2.pdf
2.2.8.6.1.2
Test
Description
2.2.8.6.1.2.1 The Roland Disability Questionnaire (RDQ) (AKA Roland-Morris Questionnaire (RMQ)) variously with 18, 23 and 24 point scale dependent upon the edition (I assume) asks the patient to check off the functional limitations imposed back and or leg pain. The RDQ that the author uses in this study is based on 24 points and is an adaptation of the Sickness Impact Profile. The greater the number of items checked by the patient the greater the disability. Improvement can be calculated as a percentage of the total number of disabling attributes before and after a series of treatments. If, for example, at the beginning of treatment, a patient’s score was 12 and, at the conclusion of treatment, her score was 2 (10 points of improvement), we would calculate an 83% improvement. (10/12=83%).
2.2.8.6.1.2.2 A score of 14 or more is considered a poor outcome. [15]
2.2.8.6.1.3 Reliability
& Usage
2.2.8.6.1.3.1 Test described [16] [17] Reliability, validity and sensitivity [18] [19] [20] [21] Usage [22] [23] [24]
2.2.8.6.1.4 Research
References
2.2.8.6.1.4.1 http://www.chirogeek.com/001_Roland-Morris-Questionnaire.htm
2.2.8.6.1.4.2 A study of the natural history
of low-back pain. Part II: development of guidelines for trials of treatment in
primary care
2.2.8.6.1.4.3 Measuring the functional status
of patients with low back pain
2.2.8.6.1.4.4 Defining the minimum level of detectable
change for the Roland-Morris questionnaire
2.2.8.6.1.4.4.1 Full Text Article
2.2.8.6.1.4.4.1.1 http://www.anatomyfacts.com/research/definingmldcroland.pdf
2.2.8.6.1.4.5 Responsiveness and minimal
clinically important difference for pain and disability instruments in low back
pain patients
2.2.8.6.1.4.5.1 Full Text Article
2.2.8.6.1.4.5.1.1 http://www.anatomyfacts.com/research/responsiveness&minimal.pdf
2.2.8.6.1.4.7 A benefit of spinal
manipulation as adjunctive therapy for acute low-back pain: a stratified
controlled trial
2.2.8.6.2
McGill Pain Questionnaire (PPI (Present Pain
Intensity)(Intensity) and PRI (Pain Rating Index)(Quality))
2.2.8.6.2.1 Test
2.2.8.6.2.1.1 Introduction
2.2.8.6.2.1.1.1 The long form of this questionnaire was used in this study. The short form has been included for your information. The scales for both these tests are ordinal (names attached to numbers which have greater than or less than values but lack equal intervals) for the purposes of deriving statistical calculations are treated as if they were interval (equal intervals between numbers).
2.2.8.6.2.1.1.2 Reference
2.2.8.6.2.1.1.2.1 http://www.anatomyfacts.com/Muscle/statsdisc.htm#scales
2.2.8.6.2.1.2 McGill Pain Questionnaire (SF-MPQ) Short Form [25]
2.2.8.6.2.1.2.1 Test
2.2.8.6.2.1.2.1.1 http://www.anatomyfacts.com/research/mcgill.pdf
2.2.8.6.2.1.2.1.2 http://www.anatomyfacts.com/research/mcgill3.pdf
2.2.8.6.2.1.2.2 Test Description Short Form
2.2.8.6.2.1.2.2.1 The short form of the McGill pain questionnaire, copyrighted by Ronald Melzack in 1984, correlates well with the long form, which was used in this study. The short form has several components e.g. Pain Rating Index (PRI), Present Pain Intensity (PPI)/Visual Analog Scale (VAS). [26]
2.2.8.6.2.1.2.2.2 The Pain Rating Index (PRI) has 11 sensory components (Throbbing, shooting, stabbing, sharp, cramping, gnawing, hot-burning, aching, heavy, tender, & splitting), and 4 affective components (tiring-exhausting, sickening, fearful, punishing-cruel) Under each component the subject is asked to rate degree of that attribute using (none=0, mild=1, moderate=2, severe=3) These 15 components spanning two areas (sensory & affective) are scored separately and then added together in a total sum.
2.2.8.6.2.1.2.2.3 The PPI score measures intensity on a 0-5 scale (0=no pain,1=mild, 2=discomforting, 3=distressing, 4=horrible, 5=excruciating). A visual analog scale (VAS) also allows the subject to place a mark between the continuum extremes of (no pain-worst possible pain). Some practitioners [27] have devised a scale which is 10 centimeters long which once the patients have marked the scale a centimeter ruler can be placed and the centimeter millimeter score can be calculated a used as a statistic; e.g Beginning score 5 centimeters 5 millimeters=5.5. A review of the literature does not reveal that this practice has been validated.
2.2.8.6.2.1.2.2.4 The VAS on the short form is exactly 10 centimeters long so that by have the client make a mark between or on the two extremes you can place a 10-centimeter ruler to determine the score. The bold numbers are the centimeters and the numbers between are the millimeters with the final score as illustrated above (5 centimeters 5 millimeters=5.5).
2.2.8.6.2.1.3 McGill Pain Questionnaire (LF-MPQ) Long Form
2.2.8.6.2.1.3.1 Need a copy
2.2.8.6.2.1.3.2 http://www.anatomyfacts.com/research/mcgill2.pdf
2.2.8.6.2.1.3.3 Test Description Long Form
2.2.8.6.2.1.3.3.1 The earlier (long form version of the McGill pain questionnaire, copyrighted by Ronald Melzack in 1970, includes four groups of descriptors (Sensory, affective, evaluative, & miscellaneous). Each of these descriptors has several attributes, which in descending order represent increased discomfort rated with the number of the tick mark in the category. For example the first number has flickering, quivering, pulsing, throbbing, beating, & pounding. If you selected pounding your rating would be 6. There are 20 descriptors each with varying numbers of attributes. Each category is totaled and the grand total is the PRI score. The score range is 0-79.
2.2.8.6.2.1.3.3.2 The PPI score is tabulated in the same way as the short form which measures intensity on a 0-5 scale (0=no pain, 1=mild, 2=discomforting, 3=distressing, 4=horrible, 5=excruciating). The visual analog scale is not included but an anterior/posterior body chart with descriptors is provided. A front and back body chart with suggested markings is also provided but no score is provided in the final totals.
2.2.8.6.2.2 Reliability
and Usage
2.2.8.6.2.2.1 Usage [28] Test Described [29] [30] [31] reliability and validity.[32] [33] [34] [35] [36] [37] Visual Analog Scale [38]
2.2.8.6.2.3 Research
References
2.2.8.6.2.3.1
http://www.chcr.brown.edu/pcoc/Physical.htm#McGill%20Pain%20Questionnaire
2.2.8.6.2.3.2
The short-form McGill Pain
Questionnaire in chronic cancer pain
2.2.8.6.2.3.3
Relationship between MPQ and VAS in 962
patients. A rationale for their use
2.2.8.6.2.3.4
The McGill Pain Questionnaire:
major properties and scoring methods
2.2.8.6.2.3.5 The short-form McGill Pain Questionnaire
2.2.8.6.2.3.6 Transcutaneous electrical nerve
stimulation for low back pain
2.2.8.6.2.3.7 The language of low back pain:
factor structure of the McGill pain questionnaire
2.2.8.6.2.3.8
Principal dimensions of the
pain experience and psychological disturbance in chronic low back pain patients
2.2.8.6.2.3.9
Factorial validity of the short-form McGill
pain questionnaire (SF-MPQ)
2.2.8.6.3
State Anxiety Index (SA) (State-Trait Anxiety Inventory
Form Y (STAI))
2.2.8.6.3.1 Test
2.2.8.6.3.1.1
Need to
get a copy
2.2.8.6.3.2
Description
2.2.8.6.3.2.1
Consists
of 40 questions 20 to assess the current anxiety state and 20 to assess the
personality traits of the individual. The test takes about 10 minutes to complete.
This instrument assesses the level induced by stressful experimental procedures
and by unavoidable real-life stressors such as imminent surgery, dental
treatment, job interviews, or important school tests. The State-Trait Anxiety
Inventory Form Y (STAI) is the definitive instrument for measuring anxiety in
adults. The STAI clearly differentiates between the temporary condition of
"state anxiety" and the more general and long-standing quality of
"trait anxiety." The essential qualities evaluated by the
STAIS-Anxiety scale are feelings of apprehension, tension, nervousness, and
worry. Scores on the STAIS-Anxiety scale increase in response to physical
danger and psychological stress, and decrease as a result of relaxation
training.” [39]
2.2.8.6.3.2.2
So far I could find no research directly
linking orthopedic movement with this test. Nor did the author cite research.
2.2.8.6.3.2.3
The
State Anxiety Index(SAI) comprises separate self-report scales to measure state
(at this moment) anxiety. Scores can range from 20 (minimal anxiety) to 80
(maximum). The norms of state anxiety for working adults are considered to be
35.7 (standard deviation [SD] 10.4) for men and 35.2 (SD 10.6) for women.
2.2.8.6.3.3 Reliability
& Usage
2.2.8.6.3.3.1 Reliability, validity and internal consistency [40] [41] [42]and widely used in research [43] in a variety of disciplines, psychology and medicine. [44] [45] [46] [47] [48]
2.2.8.6.3.4 Research
References
2.2.8.6.3.4.1 http://www.mindgarden.com/products/staisad.htm
2.2.8.6.3.4.2 http://www.cps.nova.edu/~cpphelp/STAI.html
2.2.8.6.3.4.3 Biofeedback and relaxation
training with three kinds of headache: treatment effects and their prediction
2.2.8.6.3.4.4 Failure to complete treatment for
headache: a multiple regression analysis
2.2.8.6.3.4.5.1
Full Text Article
2.2.8.6.3.4.5.1.1
http://www.anatomyfacts.com/research/statetai.pdf
2.2.8.6.3.4.6 Does experience influence perception of
dyspnea?
2.2.8.6.3.4.6.1
Full Text Article
2.2.8.6.3.4.6.1.1
http://www.anatomyfacts.com/research/statetai2.pdf
2.2.8.6.3.4.7 Literature Reviews
2.2.8.6.3.4.7.1
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?itool=pubmed_DocSum&db=pubmed&cmd=Display&dopt=pubmed_pubmed&from_uid=9621742
2.2.8.6.3.4.8 Test-retest reliabilities of
State-Trait Anxiety Inventory in a stressful social analogue situation
2.2.8.6.4
Modified Schober test (lumbar range of motion) [49]
[50]
2.2.8.6.4.1
Description
2.2.8.6.4.1.1 This is a simple but reliable objective measure of lumbar spinal range of motion, which has been extensively researched as an accurate predictor of pathology (e.g. ankylosing spondylitis) of the lower spine.
2.2.8.6.4.1.2 The test is a simple objective measurement of the distance between two points at mid distance 10 cm superior and 5 cm inferior to the PSIS midpoint during flexion and extension activities with the centimeter result recorded for both measurements. Norms have been established.
2.2.8.6.4.1.3 The Schober test has a norm of about 7 cm (SD 1.2).
2.2.8.6.4.2 Test
2.2.8.6.4.2.1 Need to get a copy
2.2.8.6.4.2.2 http://www.anatomyfacts.com/research/activities.htm#schober
2.2.8.6.4.2.3 http://moon.ouhsc.edu/dthompso/namics/labs/standing.htm
2.2.8.6.4.3 Reliability
& Usage
2.2.8.6.4.3.1 Test Described [51] [52] Norms [53] Validity, Intra observer (r = 0.99) & inter observer reliability (r = 0.97) [54] [55] [56] [57] [58] [59]usage [60] [61] [62] [63]
2.2.8.6.4.4 Research
References
2.2.8.6.4.4.1 Reproducibility of nine tests
to measure spinal mobility and trunk muscle strength
2.2.8.6.4.4.2 Defining spinal mobility in
ankylosing spondylitis
2.2.8.6.4.4.3.1 Full Text Article
2.2.8.6.4.4.3.1.1
http://www.anatomyfacts.com/research/associationbet.pdf
2.2.8.6.4.4.4 Literature Review
2.2.8.6.4.4.4.1 Keywords (modified schober)
2.2.8.6.4.4.4.1.1
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=search&DB=pubmed&cmd=Display&dopt=pubmed_pubmed&from_uid=17143634
2.2.8.6.4.4.4.2 Keywords Keywords=Moll JM, Wright V. Normal range of spinal mobility. An objective clinical study Related Articles
2.2.8.6.4.4.4.2.1
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Display&itool=abstractplus&dopt=pubmed_pubmed&from_uid=5557779
2.2.8.6.4.4.5 No Keywords Specified
2.2.8.6.4.4.5.1
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=search&DB=pubmed_DocSum&db=pubmed&cmd=Display&dopt=pubmed_pubmed&from_uid=8184354
2.2.8.6.4.4.5.2
2.2.8.6.4.4.6 Spinal mobility in ankylosing spondylitis:
reliability, validity and responsiveness
2.2.8.6.4.4.6.1 Full Text Article
2.2.8.6.4.4.6.1.1
http://www.anatomyfacts.com/research/spinalmobility.pdf
2.2.8.6.4.4.7 A randomized, double-blind,
placebo-controlled trial of sclerosing injections in patients with chronic low
back pain
2.2.8.6.4.4.7.1 Full Text Article
2.2.8.6.4.4.7.1.1
http://www.anatomyfacts.com/research/arandomized.pdf
2.2.8.7 Remarks on statistics
2.2.8.7.1
With a level of significance of 0.05 and a power
of 0.80, minimum samples of 20 subjects per group [64] (JL., 1981) were required to
detect a proportional reduction of pain of 50%. Outcome data were analyzed by
intention to treat and group means compared with ANOVA, and subsequently
Scheffé (post hoc). Minimal, insignificant differences between groups at
baseline with near normal distributions permitted analysis without adjustment.
2.2.8.8
Measures (Dependent Variables)
2.2.8.8.1 RDQ
Score (Function)
2.2.8.8.2 PPI
Score (intensity of pain)
2.2.8.8.3 PRI
Score (quality of pain)
2.2.8.8.4 State
Anxiety Index Score (SA)
2.2.8.8.5 Modified
Schober Test, cm (Lumbar Range of Motion)(ROM)
2.2.9 Treatment/Assessment Providers
2.2.9.1
Two registered massage
therapists, with more than 10 years experience, provided treatment, which was
monitored by the principal investigator (also a registered MT) for consistency
in application.
2.2.9.1.1 “Two
treatment providers were hired to deliver treatments, but it became necessary
for the principle investigator, who is also a registered massage therapist, to
provide treatment when the other providers experienced personal distress (e.g.,
death of a family member).” [65]
We do not learn when the primary treatment provider drops out of the study and
the author replaced her.
2.2.9.2
Certified personal trainer and
certified weight-trainer supervisor (this was one person?) who along with one
of the massage therapists, provided treatment for the remedial exercise and
sham laser groups provided additional treatment.
2.2.9.3
Three physiotherapists provided
the range of motion test (Schober) and were blind to which group each subject
was allocated.
2.2.9.4
Calculation of pay to providers
2.2.9.4.1 Massage
Therapists
2.2.9.4.1.1 Soft
tissue Massage
2.2.9.4.1.1.1 Two massage therapists were hired to provide the soft tissue treatments and paid $40 for each 30-35 minute session for 6 sessions. Each massage therapist then handled approximately 25 clients for 6 visits each or 150 visits over about a month’s period (37.5/clients/week or about 18.75-21.88 hours/week) to the tune of $6000 (50 x 6= 300 x 40=12000/2=$ 6000). This works out to a total of 75-87.5 patient hours in a month. At that rate the massage therapists were paid between $68.57-$80 per hour.
2.2.9.4.1.2 Sham
Laser
2.2.9.4.1.2.1 Sham Laser (20 minutes) 6 sessions $15 per session=$90
2.2.9.4.1.2.2 One massage therapist and a trainer provided sham laser treatments 25 patients received sham laser treatments
2.2.9.4.1.2.3 The massage therapist saw about 12 sham laser patients for 6 visits with a total of 72 visits at about 20 minutes for each session and made $15 per session or $1080 or about 24 hours of sham treatment in a month. This works out to about $45 per hour for sham laser treatment.
2.2.9.4.1.2.4 One certified personal trainer/weight-trainer supervisor (I assume this is just one person) was hired to provide sham laser treatment for 13 patients (I guessing they gave the extra client to the lone trainer). The 13 sham laser patients were seen for 6 visits of 20 minutes per session for a total of 78 visits for a total of 26 hours for the month or 6.5 hours per week, receiving $15 per session for a total of $ 1170.
2.2.9.4.1.3 Exercise/Postural Correction
2.2.9.4.1.3.1 One personal trainer/weight-trainer supervisor and one massage therapist was hired to provide “remedial exercise” for 25 patients each, which I assume included postural education although the study does not specify. In addition the study does not tell us which of the massage therapists provided the remedial exercise and so I will assume that it was the one who didn’t provide sham laser treatments. Each session was 15-20 minutes long and the therapists were paid $15 per session for 6 sessions totaling $90 per patient. There were 50 patients who received “remedial exercise” and the trainer/massage therapists were paid a total of $4500 or $2250 each for their services. There were a total of 300 visits or 150 visits per trainer and a total of 75-100 hours or 37.5-50 hours of training per trainer per month. This works out to about 9.38-12.5 additional hours per week at a rate of $45-$60 per hour.
2.2.9.4.1.4 Combined Treatment
2.2.9.4.1.4.1 One massage therapist then worked upwards to 27.88 hours per week or for a total of upwards of 111.5 hours total making about $7080 for their combined services providing both soft tissue massage and sham laser treatments. This averages out to about $63.50 per hour for the combined treatment.
2.2.9.4.1.4.2 The other massage therapist received just $6000 for a month of soft tissue massage as aforementioned but then received additional monies for remedial exercise of $2250 totaling $8250. This massage therapist worked upwards to 34.38 hours per week of upwards to 137.5 hours in a month. This works out to about $60 per hour for the combined treatment.
2.2.9.4.1.4.3 One certified personal trainer/weight-trainer supervisor worked upwards of 19 hours per week, 76 hours total for a total of $ 3420 for combined exercise and sham laser treatments making a total of $ 45 per hour of combined treatment.
2.2.9.4.1.5
Objective
Measurement
2.2.9.4.1.5.1 The one objective measure, the range of motion test, was conducted by 3 physiotherapists who were blind to which group each subject was allocated. The study does not tell us, however, how much the physical therapists were paid or how much time they spent completing their tasks.
2.2.9.4.1.6
Summary
2.2.9.4.1.6.1 Soft Tissue Massage=50 patients 300 visits=$12000 Exercise/Posture=50 patients 300 visits=$4500 Sham laser Treatment=25 patients 150 visits=$2250 Total=$18750 for all of the treatments provided in this research project. Massage Therapists received an average bulk payment of $ 7665 for their combined treatments working an average of 124.5 hours in a month at an average of $61.57 per hour of work with an average workweek of 31 patient hours for 4 weeks. The trainer worked upwards of 19 hours per week, 76 hours total for a total of $ 3420 for combined exercise and sham laser treatments making a total of $ 45 per hour of combined treatment.
2.2.10
College of Massage Therapists
Ontario (Registered Massage Therapists
for this Study)
2.2.10.1"The
College of Massage Therapists Ontario (the College), one of this province's
health regulatory bodies, exists to protect the public interest and to regulate
the profession of massage therapy." The word college in this case doesn't
refer to a school but to an organized body of persons engaged in a common
pursuit or having common interests or duties.
2.2.10.2"As
part of its responsibility to the public, the College sets minimum entrance to
practice requirements, administers the certification examinations and promotes continuous
quality improvement of massage therapist's knowledge, skills and abilities
through the Quality Assurance Programme."
2.2.10.3"The
College also promotes research and development of expertise in the massage
therapy profession."
2.2.10.4It
does not appear that the college actually regulates schools.
2.2.10.5The
College of Massage Therapists of Ontario regulates the massage therapy
profession through the administration of the Regulated Health Professions Act
(RHPA) and the Massage Therapy Act, (MTA) as they pertain to the classification
and practice of massage therapy in Ontario. The College of Massage Therapists
of Ontario exists to protect and serve the public by ensuring the competency
and quality of care provided by Massage Therapists through the maintenance of
Standards and Regulations. Through its activities and programmes the College
provides quality assurance and continuing education for Massage Therapists.
2.2.10.6Reference
2.2.10.6.1
http://www.cmto.com/about/cmto.htm
2.2.11
Results
2.2.11.1Most
of the clients that started the study completed it. Roughly 25 people completed
the treatments in each of the four groups with a total of 100 subjects.
2.2.11.2Findings
2.2.11.2.1
Post Treatment
2.2.11.2.1.1
Note
2.2.11.2.1.1.1RDQ=2.5 or greater is considered clinically significant.
2.2.11.2.1.2
“Massage therapy group (Group # 1) had
significantly better scores than the remedial exercise (Group # 3) (4.2) and
sham laser groups (Group # 4) (5.0) on measures of function (RDQ), intensity of
pain (PPI) quality of pain (PRI) and in addition with group 4 on State Anxiety (SA)
Group 1 also had significantly better scores than the soft-tissue manipulation
group (Group # 2) on the PPI.” [66] No significant
differences were reported by the author between Group # 1 and Groups 3 on state
anxiety. The author reported no differences between Group # 1 & 2 on any of
the following measures; RDQ, PRI, & State anxiety.
2.2.11.2.1.3
At the end of treatment (Post-treatment) the
soft-tissue manipulation group (Group # 2) had significantly better scores than
the remedial exercise (Group # 3) (2.8) and sham laser groups (Group # 4) (3.6)
on the RDQ and significantly better scores than the sham laser group (Group #
4) on the PPI. This implies no significant differences between Group # 2 and
between Groups 3 & 4 on PRI, & State anxiety and no differences reported
between group 2 and 3 on PPI (these measures were not mentioned in the study).
2.2.11.2.1.4
There were no statistical differences reported by
the author at post treatment on RDQ PPI PRI SA between Group 3 and Group 4.
2.2.11.2.1.5
There was no post treatment significant difference
in the lumbar range of motion between the groups. [67]
2.2.11.2.2
Follow-up
2.2.11.2.2.1
“At follow-up the comprehensive massage therapy
group (Group # 1) continued to have significantly improved scores over the sham
laser group (Group # 4) on the RDQ, PPI and PRI and had significantly better
scores than the remedial exercise group (Group # 3) on the RDQ and PPI.” [68] No statistical
differences were reported between group 1 and group 3 on PRI SA.
2.2.11.2.2.2
Whether the comprehensive massage therapy group
(Group # 1) had significantly improved scores at follow-up compared with the
soft-tissue manipulation group (Group # 2) is unclear. These findings seem to conflict.
2.2.11.2.2.2.1At the 1-month follow-up, 63% of the subjects in the comprehensive massage therapy group reported no pain, as compared with 27% in the soft-tissue manipulation group, 14% in the exercise group and 0% in the sham laser group. [69]
2.2.11.2.2.2.2“At follow-up there were no statistical differences between the comprehensive massage therapy group and the soft-tissue manipulation group.” [70]
2.2.11.2.2.2.3One possible interpretation is that scores from the McGill Pain Questionnaire (LF-MPQ) Long Form PPI (5 point scale for intensity-0=No Pain) were added together forming a mathematical ratio between the total number of responses with a no pain rating divided by the total responses in the group. The quotient is the percentage of respondents who reported a “No Pain” rating. This is an ordinal scale, which is treated as if it were a ratio scale. These self-rated scales are especially sensitive to bias because they are essentially subjective reports. The likelihood of a possible negatively skewed distribution given the under 30-sample size is uncertain but possible if the population is skewed (Central Limit Theorem). If Sedergreen is correct a skewed population is possible with self-reported screening. Since there was no Concealed Allocation in this study selection bias is possible as the groups were formed. Given that the researcher herself may have received monies for providing Soft-tissue manipulation to subjects, economically incentivized bias may have also been present negatively skewing the post treatment and follow-up scores of both the comprehensive massage group and the soft tissue manipulation group. The scores may have been less negatively skewed in the soft tissue manipulation group, which would mean fewer extreme no pain, scores and thus a lower percentage of subjects reporting no pain in the soft-tissue group.
2.2.11.2.2.3
At follow-up the soft-tissue manipulation group
(Group # 2) was not distinguishable from Group 3 (exercise group); both group
means were statistically better than the mean for the sham laser group (Group #
4) on the RDQ. If this is true how can Group 1 be statistically superior to
group 3 since there are no statistical differences between group 1 and group 2?
2.2.11.2.2.3.1One possible explanation is that Group 1
scores were more negatively skewed than group 2 scores but statistically equal
to group 2. Group 3 scores were less negatively skewed than group 2 scores but
statistically equal to group 2 but unequal to group 1.
2.2.11.2.2.4
No statistical difference was reported between
group 2 and group 4 or with group 3 and group 4 PPI PRI SA.
2.2.11.2.3
General
2.2.11.2.3.1
None of the groups showed significant post
treatment difference in Lumbar range of motion (ROM) (Schober) but no
difference between the groups (ROM) was reported by the author at follow-up. P-Values
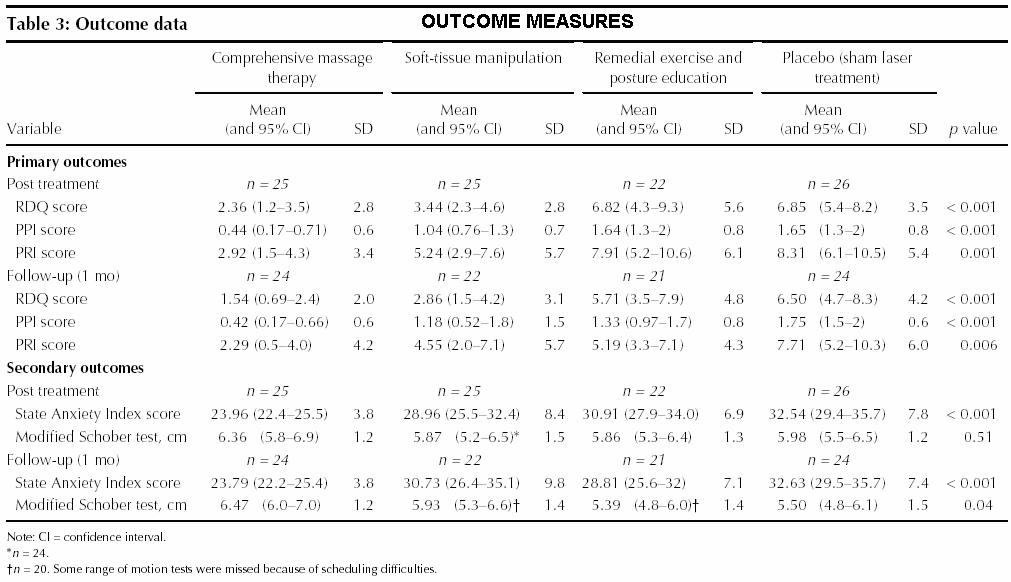
listed in Table 3 (Outcome Measures)
of the research paper indicate P-Values
of .04 for the groups at one-month follow-up. Because this is less than the
significance level of .05 a significant difference between the ROM groups at
follow-up appears to exist.
{kind=link}
2.2.11.2.3.2
Both the comprehensive massage therapy group and
the soft-tissue manipulation group showed clinical significance for the
improvement of function.
2.2.11.2.3.3
At the end of treatment and at follow-up the
comprehensive massage therapy group had significantly better scores than the
sham laser group on state anxiety, whereas no other group did.
2.2.11.2.3.4
The mean scores on the pain indexes for all of the
groups were lower at the end of treatment than at baseline.
2.2.11.2.3.5
At posttest 8% of the subjects in the sham laser
group indicated that they had no pain as compared with 5% in the exercise and
education group.
2.2.11.2.3.6
All subjects' reported levels of pain in the
comprehensive massage therapy group decreased in intensity from baseline to
post treatment, which did not occur in any other group.
2.2.11.2.3.7
Comprehensive massage therapy seemed to have the
greatest impact on pain scores but was only marginally better than soft tissue
manipulation alone for improving function.
2.2.12
Cost & Time
2.2.12.1Comprehensive
Massage Therapy= $50/session 6 Sessions=$300 Time; Soft tissue=30-35 minutes
Exercise/Postural=15-20 Total=45-55 minutes Total time=4.5 hrs-5.5 hrs Daily
exercise=Self exercise 1 x per day 2 repetitions of exercises/stretches = 15-
20 minutes (?=not specified) 7 days a week (?=not specified)=1.75 hrs per week
for 4 weeks=7 hours Undisclosed time spent on strengthening or mobility
exercises such as walking, swimming or aerobics and to build overall fitness
progressively. Total hours in one month=12.5 hours with additional time spent
on strengthening/mobility.
2.2.12.2Soft-Tissue
Manipulation= $40/Session 6 sessions=Time 30-35 minutes per session= $240 Total
Time=3.5 hours
2.2.12.3Exercise/Postural
(15-20 minutes) $15/Session 6 sessions=$90 Total=2 hours Daily exercise=Self
exercise 1 x per day 2 repetitions of exercises/stretches = 15- 20 minutes
(?=not specified) 7 days a week (?=not specified)=1.75 hrs per week for 4
weeks=7 hours Total=9 hours with additional time spent on
strengthening/mobility.
2.2.12.4Sham
Laser (20 minutes) 6 sessions $15 per session=$90
2.2.13
Limitations
2.2.13.1Single
setting
2.2.13.2Specific
soft tissue techniques by only two therapists
2.2.13.3Unmeasured
provider effects on the validity of outcome measures
2.2.13.4Limited
protocol; set number of treatments regardless of severity or complexity of the
problem and short term follow-up
2.2.14
Contact Information
2.2.14.1Michele
Preyde, Faculty of Social Work, University of Toronto, 246 Floor St. W, Toronto
ON M5S 1A1;
2.2.14.2E-Mail
2.2.14.2.1
mailto:preyde.shafir@sympatico.ca
2.2.14.3At
the time of the research
2.2.14.3.1
Michele Preyde was a PhD student in the Faculty of
Social Work, University of Toronto, and a member of the College of Massage
Therapists of Ontario, Toronto, Ont.
2.2.14.4Currently
2.2.14.4.1
Michèle Preyde, PhD, RSW Assistant Professor
Department of Family Relations and Applied Nutrition University of Guelph N1G
2W1 519-824-4120 Ext. 58599 Fax: 519-766-0691
2.3 Letters (Summarized Comments) to the Editor re: Effectiveness of
massage therapy for subacute low-back pain: a randomized controlled trial By
Michele Preyde
2.3.1 Is massage therapy genuinely effective? [71]
2.3.1.1
Lloyd Oppel Emergency physician
Vancouver, BC
2.3.1.1.1 Would
the less expensive form of massage therapy (Is there a less expensive version
in Canada) performed by non-registered therapists be as effective as the $50
version performed by registered massage therapists?
2.3.1.1.2 Sham
massage would have been a better control treatment because there is no way of
knowing whether touch from a caregiver only would reproduce the treatment
effects.
2.3.1.1.3 Volunteer
subjects may be predisposed to believe in the positive effects of massage
therapy and since the subjects were not blinded to the treatment.
2.3.1.1.4 Although
Preyde states that massage improves the patient function it would be more
accurate to say that massage improved subjects perception of improved function.
2.3.1.1.5 Self-rating
scales (self-reported measures of function, pain and state anxiety) may be less
informative for the reasons cited above than the objective range of motion
study conducted by blind assessors. The outcome indicates no difference between
groups, perhaps the more true and accurate assessment of treatment result.
2.3.1.2
Chris Sedergreen, M.D. Family
physician Coquitlam, BC
2.3.1.2.1 Dr
Sedergreen points out 6 flaws in this research
2.3.1.2.1.1 Self-reported
criteria are unreliable. (How do you know this?) This was done in the screening
process to determine eligibility. Apparently Sedergreen thinks to subjects should
all receive a physical examination.
2.3.1.2.1.2 Significant
pathology (metastatic or metabolic disease) was not excluded. Given the rarity
of this and the increased cost and budget limitations of the research project
is this really necessary?
2.3.1.2.1.3 Ages
undefined (Only mean or average score). Approaches to back pain vary with age.
2.3.1.2.1.4 The
patient of the sham laser treatment did not know the laser machine was turned
off. The operator should also have been blinded to avoid unconscious
communication of its ineffectiveness.
2.3.1.2.1.5 Analgesic
use was permitted, thus creating subsets of patients whose distribution were
not randomized.
2.3.1.2.1.6 Subjects
who may have secondary gain (compensation or avoidance behaviors) were not
screened
2.3.1.2.2 Since
the interaction between massage therapists and patient is especially vulnerable
to placebo it is the researchers doubled duty to rule out these effects.
2.3.1.3
Michele Preyde’s response
2.3.1.3.1
Lloyd Oppel’s Letter
2.3.1.3.1.1 Oppel's
suggestion of substituting sham massage for sham laser treatment was according
to Preyde good but impractical due to financial & time limitations. Why
would this take more time and cost more? Subjects were told in the
advertisements they might receive "one or more modalities" This
according to Preyde might dilute their expectations. Expectations of what? That
comprehensive massage was the therapeutic treatment.
2.3.1.3.1.2 Drop
out rates were consistent with expected rates cited in other research papers. [72] Each group had
approximately the same dropout rate (1 or 2 per group) What does this have to
do with Oppel & Sedergreen comments?
2.3.1.3.1.3 Preyde
acknowledges the limitation of self-rated measures and provider influences and
so states in the research article. She further notes in her literature review
"no study that employed a truly objective measure of subacute back pain
(e.g., laboratory investigations).
2.3.1.3.2
Chris Sedergreen’s letter
2.3.1.3.2.1 Staff
physicians approved the screening criterion. Preyde states that history taking
and physical examination (was this by a physician other than the subjects
physician) helped rule out both contraindications to massage therapy as well as
exclusion criteria. She seems to be implying a greater physicians role than was
apparent in the research. It seems poorly worded.
2.3.1.3.2.2 Preyde
doesn’t think ancillary tests are appropriate. I assume she is referring to
ruling out cancer. Can't be sure cause this passage is vague. But she does cite
the following research.[73]
2.3.1.3.2.3 As
aforementioned due to funding and time limitations this was not reported or
conducted as a double-blinded study and according to the author it was not feasible.
Why? Even still, despite the fact that the providers of both the sham laser and
exercise treatment groups believed that the exercise to be an effective remedy,
at posttest 8% of the subjects in the sham laser group indicated that they had
no pain as compared with 5% in the exercise and education group. If some
unconscious communication about the sham laser’s ineffectiveness was
communicated by the provider it was not evident in this research.
2.3.1.3.2.4 Medication
use was not considered during randomization however as it turns out patients
who were using analgesics were evenly distributed and among the groups and
within the 95% Confidence Interval of their group mean. That is to
say, the scores of the subjects using medication were not above or below the
expected sampling parameters for other members of the group.
2.3.1.3.2.5 None
of the subjects of this study were receiving any disability
payments/compensation for their low-back pain and thus would have no cause to
disavow or declare treatment effects (no secondary gain).
2.3.1.3.2.6 The
author calls for more research to provide conclusive evidence for treatment
effectiveness. A quick search does reveal some additional research in this
area. [74] [75]
2.4 Recap
2.4.1 This peer reviewed, randomized, and controlled trial of the
effectiveness of massage therapy for subacute low-back pain is the first of its
kind in the literature of massage therapy research. The research study compared
3 treatment groups with a control group. The groups were as follows; Group #
1=Comprehensive (soft tissue, exercise/postural ed), Group # 2=Soft tissue
(soft tissue only), Group # 3=exercise (exercise/postural ed) and Group # 4=one
control group (sham laser). Patients were recruited from college campus via
E-Mail, local advertisements, and physician flyers and then screened according
to self-reported criterion (subacute low-back pain (1 week-8 months), no
significant pathology, no pregnancy, stable health, previous lb pain history
ok, Positive X-Ray mild pathology ok.). Nearly 100 people, mostly overweight,
college educated women in their mid to late 40’s with non complicated low back
pain participated in the study. Subjects were, then, randomly assigned to one
of 4 groups aforementioned. The research was conducted at a multidisciplinary
facility.
2.4.2 The soft-tissue therapy was provided by two registered massage
therapists. The author of the research paper was also a registered massage
therapist who provided patient treatment when one of the other registered
massage therapists dropped out of the study due to a family emergency. The
exercise and postural education was provided by a certified personal trainer,
and certified weight-trainer supervisor. Three physiotherapists provided the
range of motion test (Schober) and were blind to which group each subject was
allocated.
2.4.3 The funding source for this project was not declared.
2.4.4 Modalities included; Soft-Tissue manipulation (friction, Trigger
points, & Neuromuscular), Exercise/Postural Correction (Lumbar/hip/thigh
stretches, waking/swimming/aerobics, postural education) Sham Laser
(Non-functioning laser)
2.4.5 Patients were evaluated on several outcome measures including; Self
reported function (RDQ), intensity (PPI) and quality (PRI) of pain, State
anxiety (pre movement anxiety)(SA), and objective lumbar range of motion
(modified Schober)(ROM).
2.4.6 Approximately 25 subjects in four groups (100 total approximately)
completed the study. Initial baseline measures were completed pre-treatment,
Post-treatment measures after 1 month (6 sessions) of treatment and follow-up
measures 1 month after treatment ended.
2.4.7 Results Summary
2.4.7.1
References
2.4.7.1.1 Worksheet
2.4.7.1.2 Groups
2.4.7.1.3 Modalities
2.4.7.1.4 Variables
2.4.7.1.5 Baseline Measures
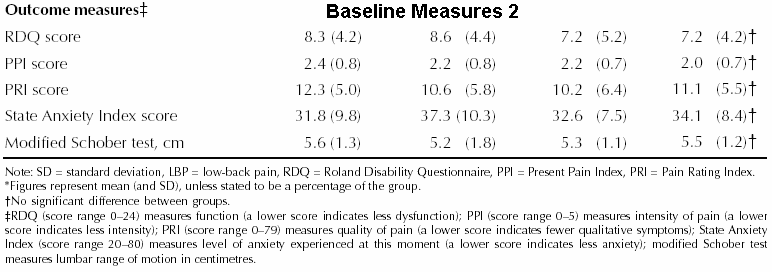{kind=link}
2.4.7.1.6 Outcome Measures
2.4.7.2
At one month follow-up there was
no statistical difference between mean scores of group 1 & 2 although the
author notes that patients in Group 1 reported a greater pain reduction than
any other group. No statistical differences, post treatment, were found between
any of the groups on the only objective ROM measure (Schober) which was also
the only measure evaluated by blinded assessors. At follow-up, P-Values, (probability that the
difference between groups is due to chance alone. If the p value is lower than
.05, for example there is significant difference between two or more groups)
reveal significant differences between the groups for the ROM (Schober) measure
(Outcome Measures) but the author
does not reference or explain this result. Group 1 was superior to all of the
groups post treatment for PPI and remained so at follow up compared to groups 3
& 4. Likewise Group 1 was superior
to groups 3 & 4 both post treatment and follow up on RDQ and superior on
PRI post treatment to groups 3 & 4.
Group 1 continued to remain more effective than group 4 on PRI at follow
up.
2.4.7.3
Group 2 was superior post treatment to both groups 3 & 4
on RDQ but only to group 4 on PPI. At follow up group 2 continued to be more
effective than group 4 on RDQ but there was no statistical difference between
groups 2 & 3 at follow up. As aforementioned no statistical difference
between groups 1 & 2 was present at follow up. Does it not follow that
there is no statistical difference between group 1 and 3 at follow up? As
previously stated group 1 was found to be statistically superior to group 3 at
follow up. The author does not explain this apparent anomaly.
2.4.7.4
Group 3 was superior to group 4 on RDQ at follow up.
2.5 Critical Analysis
2.5.1 The comprehensive massage therapy group was statistically indistinct
from the soft tissue group, which was statistically matched with the exercise
group at follow up. All three groups were better at follow-up than the control
group. More comprehensive massage therapy subjects reported no pain at follow
up than in any other group. It remains unclear how the aforementioned pain/no
pain ratings were calculated while overall statistical differences (including
pain rating PPI PRI) were statistically indistinct. None of the treatment groups
improved objective range of motion at post treatment. It remains unclear if
this was also true at follow up.
2.5.2 These findings may inform prospective therapists and clients when
considering various treatments for low back pain. Certainly any of these treatments
would be more effective than doing nothing. Given that any of the three
treatments would provide relatively equal relief from pain and improved
perceived function (RDQ) other evaluative factors such as time and cost may
be considered.
2.5.3 Comprehensive Massage costs $300 for 6 sessions over a month period
totalling 12.5 hours with additional time spent on strengthening/mobility self
exercise. Soft-Tissue Manipulation costs $240 for 6 sessions over a month
period totalling 3.5 hours without additional time commitment.
Exercise/Postural costs $90 with a total of 7 hours with additional time spent
on strengthening/mobility.
2.5.4 The least time consuming option for clients would be soft tissue
treatment and the least expensive would be exercise/postural correction. The
comprehensive massage therapy may provide better pain relief, 1 month after
treatment, but is the most expensive and time consuming of the treatment
modalities. The comprehensive massage group provided neither statistically
significant different results than soft tissue manipulation on either
self-rated function or pain indexes (PPI PRI).
2.5.5 The validity of this research is compromised by several factors. The
author of the research study was herself a registered massage therapist who
provided some of the treatments to subjects in the study. Registered massage
therapists in this study were hired to provide soft tissue treatments to
subjects. It may be that the author of the study also received monetary
compensation for her soft tissue therapy. The author of the study was herself a
member of the College of Massage Therapists of Ontario Canada (College of Massage Therapists) which has as its mission
statement "All qualified massage therapists are registered and proud to be
associated with the College" In her summary conclusion the author states
"Patients with subacute low-back pain were shown to benefit from massage
therapy, as regulated by the College of Massage Therapists of Ontario and
delivered by experienced massage therapists." [76] This is seems
inconsistent with the authors own conclusions within the body of the research
study namely;
2.5.5.1
“At follow-up there were no statistical
differences between the comprehensive massage therapy group and the soft-tissue
manipulation group.” [77]
2.5.5.2
“by follow-up there was no
statistical difference between the soft-tissue manipulation group and the
remedial exercise group.” [78]
2.5.6 Why did the author
find it necessary to mention “College of Massage Therapists” in her summary
conclusion when regulation of massage technique & the experience of the
massage therapists are not measured dependent variables in this research?
2.5.7 Did the College of
Massage therapists register the registered experienced massage therapists in
this research study? It is unknown what the source of
funding for the study was. If the college of massage therapists funded this
study, obvious bias would be more evident. Similar emphasis of place of
educational certification was not placed on the other providers of treatment in
this research study e.g. personal trainer, weight-trainer
supervisor & physiotherapists. We do not learn for example that their
training/registration/certification/schooling benefited the outcome of the
research. It might be noted that this study does not examine relative
effectiveness of massage training programs and the author does not provide
citations as to the increased relative effectiveness of programs endorsed by
the College of massage therapists. Is there bias in this research which may
have been transmitted to the subjects (subjects use self-rating of pain and
function which may be influenced by therapeutic bias) by the proud registered
massage therapy providers (the author included) who at least in the case of the
author were a member of the college of massage therapists? Since the author
herself performed some of the massage treatments the appearance of bias is
certain whether or not its effect of subjects self-rated symptoms can be
statistically proven. If the author received only part of the compensation due
her primary therapist for treatment to the subjects it still might have been a
sizable sum of the $ 6000 due (50 x 6= 300 x 40=12000/2=$ 6000) Future studies
would benefit by having standby therapists who can provide treatment to avoid
the appearance of economically incentivized bias and easy dismissal of the
results by the scientific community.
2.5.8 Several other factors affect the validity of this
research, which received a total of 6 out of 10 by Pedro’s rating scale. The
following problems were noted;
2.5.8.1
The assignment person should be
unaware of which groups subjects are assigned to. (Concealed Allocation)
2.5.8.2
The subjects should be unaware
of whether or not they were placed in a therapeutic group (Blinded subjects)
2.5.8.3
The therapists should be unaware
that they are providing the therapeutic treatment. (Blinded therapists)
2.5.8.4
All the subjects should be
statistically analyzed whether they dropped out of the study or not. (Intention to Treat)
2.5.9 The author herself acknowledges limitations of this study (Limitations);
varied settings, varied therapists, blind therapists, protocol to fit problem
severity/complexity with long term follow up.
2.5.10
Other authors have also noted
problems with this study
2.5.10.1Lloyd Oppel M.D.
questions the effectiveness of registered massage therapist vs. non-registered
therapists, advises the use of sham massage instead of sham laser as a control,
advises blinding subjects, self rated function is not the same as actual
function, ultimately this study failed to demonstrate any improvement in actual
function which implicates the result of not blinding subjects/therapists.
2.5.10.2Chris Sedergreen,
M.D. Improper screening which should have included physician
examination (self-reported criteria unreliable), Significant pathology should
be ruled out (cancer), Vary treatment to age appropriate, blind the operator of
sham laser, analgesic use nullified randomization, disability compensated
patients with secondary gain not screened, massage therapist/client
relationship especially vulnerable to placebo effects which this study did not
seek to dilute.
2.5.10.3Michele Preyde
2.5.10.3.1
Oppel
2.5.10.3.1.1
Sham
massage good idea but impractical, subjects were told they would receive one or
multiple modalities which would dilute expectations, Drop out rates consistent
with other studies, no previous studies used truly objective laboratory
investigations.
2.5.10.3.2
Sedergreen
2.5.10.3.2.1
Staff
physicians developed screening criterion/independent examination, ancillary
tests inappropriate, not intended or reported as a double blind and control
group had higher no pain ratings thus dispelling placebo, patients using
analgesics were evenly distributed and their scores statistically similar to
non-medicated, none of the subjects were receiving disability payments, and
more research is needed.
2.5.11
All of the statistics of this
study are based on 4 self-rated/subject-rated measures (RDQ (RMQ)), PPI,
PRI, & State Anxiety) and one objective measurement (Schober).
As Lloyd
Oppel M.D. cautions, these self rated measures are "very prone
to non-specific provider influences." [79]
and as Chris Sedergreen, M.D. reminds "interaction between a
massage therapist and a patient is particularly vulnerable to producing a
placebo response, in which case the obligation of researchers in this field to
disprove such bias is substantially increased. (e.g., laboratory
investigations)." [80]
Michele
Preyde notes "Oppel’s concerns about the accuracy of reporting
the self-rated measures and the possible provider influence on subjects’
perceptions are valid" "In my review of the literature I found no
study that employed a truly objective measure of subacute back pain (e.g.,
laboratory investigations)." [81]
The following measures are discussed in more detail;
2.5.11.1Roland Disability Questionnaire (RDQ) simply measures self reported disability caused by back and or leg
pain on a 24 point scale which as more items are checked indicates greater
disability or as fewer items with progressive treatment can determine progress
in simple percentage terms. This instrument is widely used and researched for reliability,
validity and sensitivity the results of which indicate its effectiveness as a
sensitive accurate measure.
2.5.11.2McGill Pain Questionnaire (LF-MPQ) Long Form
measures self reported quality of pain over four categories; Sensory,
affective, evaluative, & miscellaneous with descriptors giving a grand
total PRI score. Also included is an intensity of pain score on a 0-5 scale.
This test is also widely used and well researched for reliability, internal
consistency, reproducibility, validity, responsiveness, and interpretability.
2.5.11.3State Anxiety Index (SA)
measures the current anxiety state (20 questions), which in this study is used
to determine whether a person is anxious prior to lumbar movement. As treatment
progresses the anxiety prior to low back movements should decrease as pain and
discomfort with lumbar movement decreases.
This psychometric instrument also measures a person’s trait anxiety (20
questions), which is part of their personality. Both scores (40 questions) are
used in this research study. Although the State-Trait Anxiety Inventory
Form Y (STAI) is one of the most widely used and validated instruments, nothing
appears in the literature supporting its use to measure anxiety prior to
orthopedic movements.
2.5.11.4Modified Schober test
is an objective measurement of spinal flexion and extension recorded in
centimetres. The three physical therapists that were hired to record these
measurements did not know which subjects were in which groups and therefore
were blinded and thus less likely to influence the test which involved the
actual measurement of spinal movement. This particular test is well-researched and reliable
objective measure of lumbar range of motion.
2.6 Conclusion
2.6.1 This study found that Comprehensive massage therapy was no better than
soft tissue massage at follow-up and soft tissue about the same as
exercise/postural education. All of the groups were better than sham laser.
Consumer decisions regarding treatment selection should be based on time and
cost. The least time consuming option for clients would be soft tissue treatment
and the least expensive would be exercise/postural correction. The
comprehensive massage therapy may provide better pain relief (although
potential bias and questionable statistics makes for an uncertain result) but
is both more expensive and time consuming than the other alternatives.
2.6.2 Validity problems were evident in this study when the researcher
herself provided and may have been paid to provide direct treatment to subjects
and then reported unusual results in the summary conclusion, which did not fit
the data (details).
The researcher included what appeared to be a “plug” to an institution she was
a member of and which may have funded the research. The author has been
contacted to verify the source of the funding along with other questions. (Questions to
Author)
2.6.3 Other validity questions include
no concealed allocation which means that the subject assignment person was not
blinded from knowing which subjects were assigned to which groups (details).
Since both therapists and subjects were also not blinded along with the
aforementioned author actually treating the patients this study had the
appearance of bias. Since self-rated measures of function, pain and anxiety are
especially susceptible to bias (Oppel)(Sedergreen) the results of this study are questionable. The statistical analysis the
researcher may have used to justify the summary “plug” involved treating a
subjective self-rating ordinal scale as if it were a ratio scale (Scales).
I could find no research to verify the validity of the McGill PPI scale used as a ratio
scale. The author has been queried on this matter. (Questions to Author)
2.6.4 Given the
possibility of bias introduced into this study it also possible that although
the distribution of the population of subjects for this study may have been
normal (Central Limit
Theorem) the group distributions may be skewed if their was
selection bias by the assignment person (choosing less severe cases for some
groups). In addition the researcher herself provided direct treatment to
subjects and may have biased subjects responses. This might explain how a
greater percentage of subjects in the Comprehensive Massage group selected no
pain rating on the PPI McGill Scale (Details). Although all of the
groups, including the exercise/postural group had a registered massage
therapists (including the author) providing treatment but the exercise/postural
group had the lowest percentage of no pain ratings.
2.6.5 If it turns out that the funding source was the College of Massage
therapists the “plug” the author placed in the summary invites further
question. Does this reflect the realities of “doing business” in producing
research for institutions and businesses that pay a lot of money for the
results they want. Does doing business as a researcher mean you have to at
least provide a gratuitous “quotable quote” in the summary abstract? How would you
like to be the person (in the business/institution) who approved the research
grant only to get back a negative research finding for your project? Your
judgement would be questioned. Likely pressure would be placed on the
researcher to give some positive findings. Future research grants may depend on
the researchers willingness to bend and spin the results into a positive
project “Plug”. This is a tough problem to assess because much of this
influence may be unwritten, unspoken, but well understood in the research
community. This is the big elephant in the room no one wants to talk about.
More study should determine how widespread this practice is because it does
erode at public trust if research becomes only an extension of marketing. As
for this research it gives the appearance of just such a “Plug”.
2.6.6 If all this is true it may be necessary to go beyond reading just the
abstract summary when reviewing research and doubly important to establish the
funding source. In addition, an understanding of basic statistical concepts
would be necessary to separate truth from spin. Research, if funded, by
independent organizations such as the Massage Therapy Foundation
may be less inclined towards this bias. This may be less about the unethical
behavior of individuals but rather a system, which encourages and rewards this
behavior. It might be counter productive, for example, to single out the author
of this study, if the problem is wide spread. As for this particular study more
information is needed before a final judgement can be reached, but the
questions raised may be worth asking in any case.
3 Research
References
3.1 Research Literacy
(Summary of Concepts)
3.1.1 http://www.anatomyfacts.com/research/literacy.htm#references
3.2 Baseline Data (Initial pre-treatment measures)
3.2.1 Baseline Measures
3.3 Outcome Measures
3.3.1 Outcome Measures
3.4 Work sheet Results
3.4.1 http://www.anatomyfacts.com/Research/Massage
Journal Club/November06/outcome.htm
9061/300= 30.20
Reviewed article 1815-1820=5
Words=4607 Citation apa = (Author,
|Year|, p.^pp. Cited Pages|) start each ref Bibliography Number.
Massage
4
Bibliography
[1-57]
Bibliography
1. Andrade, L., Gorenstein, C., Vieira Filho, A. H., Tung, T. C., & Artes, R. (2001). Psychometric properties of the Portuguese version of the State-Trait Anxiety Inventory applied to college students: factor analysis and relation to the Beck Depression Inventory. Braz J Med Biol Res, 34(3), 367-374.
2. Authors, M. (Jan 2007.). State-Trait Anxiety Inventory.
from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?itool=pubmed_docsum&db=pubmed&cmd=display&dopt=pubmed_pubmed&from_uid=9621742
3. Authors, M. (January 11, 2007). Literature Review-Modified Schober test=Key words=modified schober. from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=search&DB=pubmed&cmd=Display&dopt=pubmed_pubmed&from_uid=17143634
4. Authors, M. (January 12, 2007). Literature Review-Schober-Key words=unknown PMID=8184354. from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=search&DB=pubmed&cmd=Display&dopt=pubmed_pubmed&from_uid=8184354
5. Authors, M. (January 12, 2007). Literature Review Keywords=Moll JLiterature Review Keywords=MollM, Wright V. Normal range of spinal mobility. An objective clinical study Related Articles. Retrieved January 12, 2007, from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Display&itool=abstractplus&dopt=pubmed_pubmed&from_uid=5557779
6. Blanchard, E. B., Andrasik, F., Neff, D. F., Arena, J. G., Ahles, T. A., Jurish, S. E., et al. (1982). Biofeedback and relaxation training with three kinds of headache: treatment effects and their prediction. J Consult Clin Psychol, 50(4), 562-575.
7. Cd., S. (1983). State-trait anxiety inventory for adults. Palo Alto California: Mind Gardens.
8. Cherkin, D. C., Deyo, R. A., Battie, M., Street, J., & Barlow, W. (1998). A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med, 339(15), 1021-1029.
9. Cole, B., Finch, E., Gowland, C., & Mayo, N. (1995). Physical rehabilitation outcome measures: Baltimore: Williams & Wilkins.
10. Dechow, E., Davies, R. K., Carr, A. J., & Thompson, P. W. (1999). A randomized, double-blind, placebo-controlled trial of sclerosing injections in patients with chronic low back pain. Rheumatology (Oxford), 38(12), 1255-1259.
11. Deyo, R. A. (1988). Measuring the functional status of patients with low back pain. Arch Phys Med Rehabil, 69(12), 1044-1053.
12. Dudgeon, D., Raubertas, R. F., & Rosenthal, S. N. (1993). The short-form McGill Pain Questionnaire in chronic cancer pain. J Pain Symptom Manage, 8(4), 191-195.
13. Fitzthum, J. (1998). Proving the Existence of Chronic Pain Wiley Expert Witness Update: New Developments in Personal Injury Litigation. 5.1-5.20.
14. Flick, S. (Rev1988). Managing attrition in clinical research. Clin Psychol, 8, 499-515.
15. Furlan, A. D., Brosseau, L., Imamura, M., & Irvin, E. (2002). Massage for low-back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine, 27(17), 1896-1910.
16. Furlan, A. D., Brosseau, L., Imamura, M., & Irvin, E. (2002). Massage for low back pain. Cochrane Database Syst Rev(2), CD001929.
17. Hadler, N. M., Curtis, P., Gillings, D. B., & Stinnett, S. (1987). A benefit of spinal manipulation as adjunctive therapy for acute low-back pain: a stratified controlled trial. Spine, 12(7), 702-706.
18. Hart, J. D. (1982). Failure to complete treatment for headache: a multiple regression analysis. J Consult Clin Psychol, 50(5), 781-782.
19. Haywood, K. L., Garratt, A. M., Jordan, K., Dziedzic, K., & Dawes, P. T. (2004). Spinal mobility in ankylosing spondylitis: reliability, validity and responsiveness. Rheumatology (Oxford), 43(6), 750-757.
20. Hollis, S., & Campbell, F. (1999). What is meant by intention to treat analysis? Survey of published randomised controlled trials. Bmj, 319(7211), 670-674.
21. Hsieh, C. Y., Phillips, R. B., Adams, A. H., & Pope, M. H. (1992). Functional outcomes of low back pain: comparison of four treatment groups in a randomized controlled trial. J Manipulative Physiol Ther, 15(1), 4-9.
22. Hyytiainen, K., Salminen, J. J., Suvitie, T., Wickstrom, G., & Pentti, J. (1991). Reproducibility of nine tests to measure spinal mobility and trunk muscle strength. Scand J Rehabil Med, 23(1), 3-10.
23. Jenkinson, T. R., Mallorie, P. A., Whitelock, H. C., Kennedy, L. G., Garrett, S. L., & Calin, A. (1994). Defining spinal mobility in ankylosing spondylitis (AS). The Bath AS Metrology Index. J Rheumatol, 21(9), 1694-1698.
24. Lachin, J. M. (2000). Statistical considerations in the intent-to-treat principle. Control Clin Trials, 21(3), 167-189.
25. Lauridsen, H. H., Hartvigsen, J., Manniche, C., Korsholm, L., & Grunnet-Nilsson, N. (2006). Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients. BMC Musculoskelet Disord, 7, 82.
26. Majani, G., Tiengo, M., Giardini, A., Calori, G., De Micheli, P., & Battaglia, A. (2003). Relationship between MPQ and VAS in 962 patients. A rationale for their use. Minerva Anestesiol, 69(1-2), 67-73.
27. Martinez-Moragon, E., Perpina, M., & Belloch, A. (2006). [Does experience influence perception of dyspnea?]. Arch Bronconeumol, 42(4), 171-174.
28. McCreary, C., Turner, J., & Dawson, E. (1981). Principal dimensions of the pain experience and psychological disturbance in chronic low back pain patients. Pain, 11(1), 85-92.
29. Melzack, R. (1975). The McGill Pain Questionnaire: major properties and scoring methods. Pain, 1(3), 277-299.
30. Melzack, R. (1983). The mcgill pain questionnaire. in: pain measurement and assessment. New York: Raven Press.
31. Melzack, R. (1987). The short-form McGill Pain Questionnaire. Pain, 30(2), 191-197.
32. Melzack, R., Vetere, P., & Finch, L. (1983). Transcutaneous electrical nerve stimulation for low back pain. A comparison of TENS and massage for pain and range of motion. Phys Ther, 63(4), 489-493.
33. Moll, J. M., & Wright, V. (1971). Normal range of spinal mobility. An objective clinical study. Ann Rheum Dis, 30(4), 381-386.
34. Oppel, L. (2000). Is massage therapy genuinely effective? Cmaj, 163(8), 953; author reply 953-954.
35. Pope, M. H., Phillips, R. B., Haugh, L. D., Hsieh, C. Y., MacDonald, L., & Haldeman, S. (1994). A prospective randomized three-week trial of spinal manipulation, transcutaneous muscle stimulation, massage and corset in the treatment of subacute low back pain. Spine, 19(22), 2571-2577.
36. Preyde, M. (2000). Effectiveness of massage therapy for subacute low-back pain: a randomized controlled trial. Cmaj, 162(13), 1815-1820.
37. Prieto, E. J., Hopson, L., Bradley, L. A., Byrne, M., Geisinger, K. F., Midax, D., et al. (1980). The language of low back pain: factor structure of the McGill pain questionnaire. Pain, 8(1), 11-19.
38. Reading, A. (1979). A comparison pain rating scales. J Psychosom Res, 24, 119-124.
39. Reading, A. E. (1980). A comparison of pain rating scales. J Psychosom Res, 24(3-4), 119-124.
40. Reading, A. E. (1982). A comparison of the McGill Pain Questionnaire in chronic and acute pain. Pain, 13(2), 185-192.
41. Roland, M., & Morris, R. (1983). A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine, 8(2), 141-144.
42. Roland, M., & Morris, R. (1983). A study of the natural history of low-back pain. Part II: development of guidelines for trials of treatment in primary care. Spine, 8(2), 145-150.
43. Rosser W., S. S. (1998). Evidence-based family medicine: Hamilton: BC Decker.
44. Rule, W. R., & Traver, M. D. (1983). Test-retest reliabilities of State-Trait Anxiety Inventory in a stressful social analogue situation. J Pers Assess, 47(3), 276-277.
45. Schulz, K. F., & Grimes, D. A. (2002). Allocation concealment in randomised trials: defending against deciphering. Lancet, 359(9306), 614-618.
46. Sedergreen, C. (2000). Is massage therapy genuinely effective? Cmaj, 163(8), 953; author reply 953-954.
47. Spielberger, C. (1983). State-trait anxiety inventory for adults. Palo Alto Calif: Mind Gardens.
48. Spielberger, C. (1989). State-trait anxiety inventory: a comprehensive bibliography. Palo Alto (ca): Consulting Psychologists Press.
49. Spielberger, C. D. (Jan 2007). State-trait Anxiety Inventory For Adults from http://www.mindgarden.com/products/staisad.htm
50. Spielberger CD, G. R., Lushene RE. (1970). Manual for the State-Trait Anxiety Inventory. Palo Alto (CA).
51. Stratford, P. W., Binkley, J., Solomon, P., Finch, E., Gill, C., & Moreland, J. (1996). Defining the minimum level of detectable change for the Roland-Morris questionnaire. Phys Ther, 76(4), 359-365; discussion 366-358.
52. W Rosser, S. S. (1998). Evidence-based family medicine: Hamilton: BC Decker.
53. Wanders, A., Landewe, R., Dougados, M., Mielants, H., van der Linden, S., & van der Heijde, D. (2005). Association between radiographic damage of the spine and spinal mobility for individual patients with ankylosing spondylitis: can assessment of spinal mobility be a proxy for radiographic evaluation? Ann Rheum Dis, 64(7), 988-994.
54. Wright, K. D., Asmundson, G. J., & McCreary, D. R. (2001). Factorial validity of the short-form McGill pain questionnaire (SF-MPQ). Eur J Pain, 5(3), 279-284.
55. Yeomans S, L. C. (1996). Functional Capacity Evaluation and Chiropractic Case Management. . Top Clin Chiro 3(3), 15-25.
56. Yeomans S, L. C. (1996). Quantitative functional capacity evaluation: the missing link to outcomes assessment. Top Clin Chiro, 3(1), 32 - 43.
57. Yeomans S, L. C. (Summer 1997). Applying Outcomes Management into Clinical Practice. J. Neuromusculoskel. System, 5(2), 1-14.